Impact of neuronal cross-talk and anomalous innervation on neuromonitoring signals in head and neck surgery
Article information

Abstract
Intraoperative neuromonitoring is widely utilized in head and neck surgery to identify and preserve the recurrent laryngeal nerve (RLN) and superior laryngeal nerve (SLN) during thyroid and parathyroid procedures. However, anatomical variations and neuronal cross-talk can complicate the interpretation of electrophysiological signals, leading to false-positive or false-negative intraoperative feedback. This narrative review evaluates literature from PubMed and Google Scholar regarding the characteristics of the non-recurrent laryngeal nerve (NRLN), laryngeal anastomotic networks (e.g., anastomosis of Galen), and sympathetic-vagal communications. The reviewed literature indicates that structural neural variations alter standard electromyographic profiles. Specifically, the NRLN frequently exhibits a shortened latency during proximal vagal stimulation due to its altered anatomical trajectory. Furthermore, neural cross-talk between the SLN and RLN via the anastomosis of Galen may produce compensatory compound muscle action potentials, potentially masking distal focal nerve injuries. Inadvertent stimulation of the cervical sympathetic trunk mimics vagal signals, presenting as atypical waveforms with variable stimulation thresholds and morphological stability. Understanding these electrophysiological features is essential for accurate intraoperative decision-making. Careful observation of latency shifts, waveform morphology, and stimulation thresholds, when integrated into standardized monitoring protocols, assists in mitigating risks associated with neural variations.
Introduction
Intraoperative neuromonitoring (IONM) has significantly advanced head and neck surgery, particularly in thyroid and parathyroid procedures. Meticulous visual nerve identification remains the cornerstone of surgical practice. However, IONM provides real-time electrophysiological feedback to assist in early neural mapping, confirm functional integrity, and prognosticate postoperative vocal fold mobility [1]. Organizations such as the International Neural Monitoring Study Group (INMSG) have introduced standardized guidelines over the past two decades [2]. Consequently, IONM is now a widely recognized tool for reducing the incidence of iatrogenic vocal fold paralysis [3].
Despite these advancements, clinicians occasionally encounter scenarios where electromyographic (EMG) signals contradict visual anatomical assessments. A primary factor in this intraoperative ambiguity is the inherent anatomical variability of the cervical peripheral nervous system [4]. The neural architecture in the neck frequently features collateral branches, variable trajectories, and internal communications between distinct networks. The presence of these atypical neural circuits can cause standard electrical stimulation to yield unexpected compound muscle action potentials (CMAPs) [5,6].
For instance, an anastomotic network might artificially maintain a robust CMAP amplitude despite a focal nerve injury. This phenomenon could provide false reassurance to the surgical team. Conversely, adjacent non-motor structures may inadvertently conduct electrical current to the laryngeal musculature [7]. This conduction can generate false-positive signals that misguide the surgical dissection. Among these structural deviations, the non-recurrent laryngeal nerve (NRLN) and internal neural communications—such as the anastomosis of Galen—have garnered significant clinical attention. Their presence may confound established neuromonitoring algorithms [8-10].
This article presents a narrative review of the literature concerning the impact of neuronal cross-talk and anomalous innervation on IONM signals. By reviewing the intersection of surgical anatomy and electrophysiology, this paper details the specific EMG signatures associated with these variations. It also discusses practical, evidence-based troubleshooting strategies intended to enhance the safety of nerve-sparing surgeries.
Literature Search Strategy
A literature search was conducted using the PubMed and Google Scholar databases to retrieve relevant articles published between 1994 and March 2026. The primary search terms included "intraoperative neuromonitoring," "thyroidectomy," and "electromyography." To specifically target the anatomical scope of this review, these primary terms were paired with secondary keywords: "non-recurrent laryngeal nerve," "vagal short latency," "anastomosis of Galen," "laryngeal neural cross-talk," "sympathetic-vagal communication," "waveform polyphasia," and "stimulation threshold." The selection criteria prioritized clinical cohort studies, anatomical cadaveric investigations, and electrophysiological case reports that evaluated latency shifts, morphological changes in CMAPs, and intraoperative troubleshooting algorithms. When multiple types of evidence were available on a given topic, clinical cohort studies and prospective electrophysiological data were weighted more heavily than isolated case reports or purely cadaveric findings. Studies focused exclusively on the engineering design of continuous intraoperative neuromonitoring (C-IONM) equipment, without reference to clinical anatomical variations, were excluded. This strategy was designed to compile representative clinical and anatomical evidence for a narrative review, rather than to perform a formal systematic review.
Anatomical Variations in Head and Neck Nerves
The conventional surgical approach to the central neck compartment relies heavily on established anatomical landmarks, such as the tracheoesophageal groove and the inferior thyroid artery [11]. However, anatomical literature highlights that variations such as the NRLN, complex laryngeal anastomoses, and sympathetic-vagal communications frequently alter these standard surgical relationships [11,12]. The major anatomical variations and neural communications relevant to atypical IONM findings are summarized schematically in Figure 1.
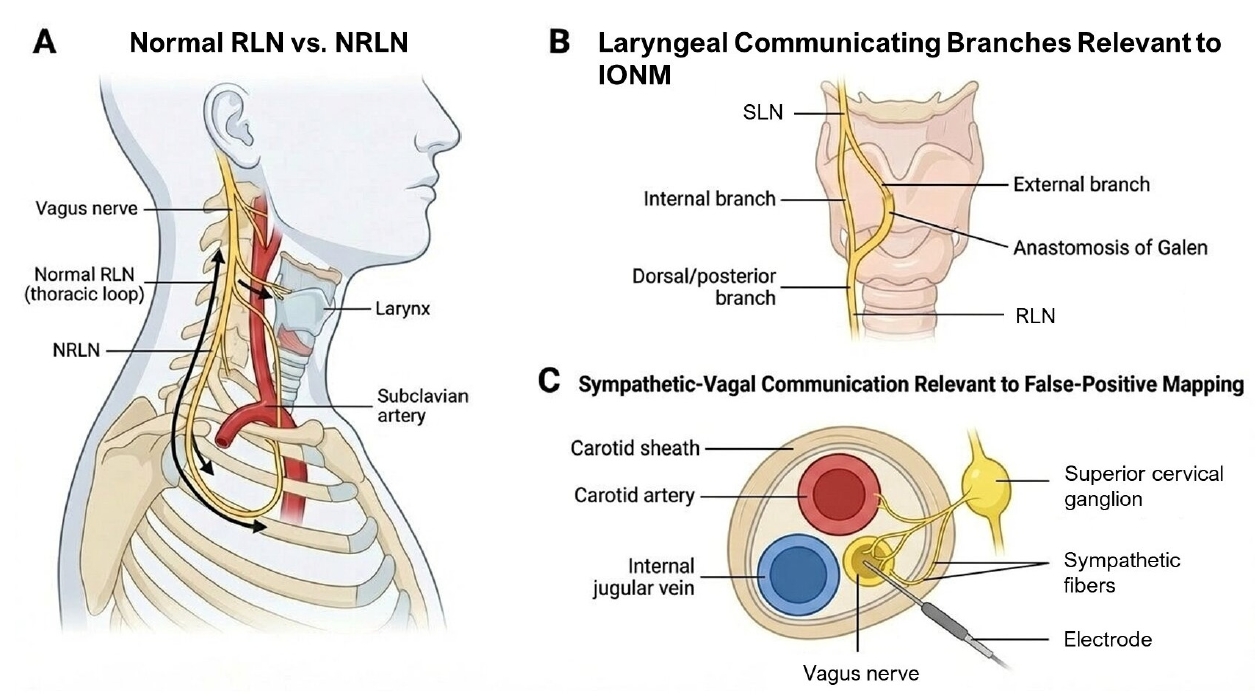
Major anatomical variations and neural communications relevant to intraoperative neuromonitoring during thyroid and parathyroid surgery. (A) Comparison of the normal RLN and the NRLN. Unlike the normal RLN, which descends into the thorax and then returns to the larynx, the NRLN arises directly from the cervical vagus nerve and follows a direct cervical course to the larynx. (B) Laryngeal communicating branches between the SLN and RLN, including the anastomosis of Galen, which may contribute to collateral conduction and atypical electromyographic findings. (C) Sympathetic-vagal communication within or adjacent to the carotid sheath, which may provide an anatomical basis for false-positive vagal mapping during IONM. RLN, recurrent laryngeal nerve; NRLN, non-recurrent laryngeal nerve; SLN, superior laryngeal nerve; IONM, intraoperative neuromonitoring.
1. The non-recurrent laryngeal nerve
The NRLN is a clinically significant variation due to its transverse trajectory. This path directly crosses typical surgical dissection planes during thyroid lobectomy [13,14]. Embryologically, the anomaly is linked to a vascular malformation during branchial arch development. Specifically, the abnormal involution of the fourth right aortic arch prevents the normal origin of the right subclavian artery [15]. This disruption results in an aberrant right subclavian artery (arteria lusoria) that arises directly from the aortic arch and courses retroesophageally. Consequently, the right recurrent laryngeal nerve (RLN) lacks the normal subclavian tether required to pull it into the upper mediastinum during fetal elongation. Instead, it branches directly from the cervical vagus nerve [16,17].
Epidemiological studies report that right-sided NRLNs occur in approximately 0.3% to 1.6% of the general population [13]. Left-sided NRLNs are exceptionally rare, with an estimated incidence of less than 0.04%, requiring the presence of situs inversus totalis accompanied by a right-sided aortic arch [18]. Morphologically, the NRLN is heterogeneous and has been classified into several subtypes based primarily on the height of its origin from the vagus nerve and its anatomical trajectory [19]. Generally, Type I NRLNs originate high in the cervical vagus and take a descending course toward the larynx. Type II NRLNs branch at a lower level from the vagus, taking a more transverse or slightly ascending path to reach the laryngeal entry point [19-21]. This morphological diversity implies that visual identification alone is highly challenging [17].
2. Laryngeal anastomotic networks
In addition to major trajectory deviations, micro-anatomical neural cross-talk adds a layer of complexity to the cervical region. The laryngeal neural network contains several documented communicating branches [22]. The most prominent is the anastomosis of Galen (ramus anastomoticus), which connects the dorsal branch of the RLN with the internal branch of the superior laryngeal nerve (SLN). For decades, this anastomosis was categorized as a purely sensory and autonomic connection transmitting proprioceptive information to the laryngeal mucosa [8,23].
However, emerging histological studies and contemporary electrophysiological mapping reports suggest that motor fibers might occasionally be shared within this connection, although direct functional confirmation in vivo remains limited. If motor fibers are indeed shared between the SLN and the RLN via the anastomosis of Galen, the intrinsic laryngeal musculature may theoretically receive functional dual innervation; however, this concept is largely extrapolated from cadaveric and small-sample electrophysiological observations rather than from large-scale clinical trials [23]. Furthermore, other connections, such as the human communicating nerve connecting the external branch of the SLN to the RLN, have been documented in cadaveric studies. If robustly developed, these anastomotic networks are hypothesized to serve as collateral motor pathways that could potentially bridge localized nerve injuries, though this remains a theoretical consideration supported primarily by anatomical and case-level electrophysiological evidence [24].
3. Sympathetic-vagal communications
Another relevant clinical scenario involves the anatomical proximity of the vagus nerve and the cervical sympathetic trunk [25]. The sympathetic trunk courses longitudinally within the prevertebral fascia, strictly parallel to the posterior aspect of the carotid sheath. In many individuals, the sympathetic trunk shares deep fascial connections or is intimately adherent to the posterior wall of the sheath containing the vagus nerve [26].
The sympathetic network possesses communicating branches (rami communicantes) that connect with lower cranial nerves. Consequently, some reports hypothesize that this structural proximity might provide a physical pathway for electrical current conduction between the sympathetic trunk and the vagus nerve during surgical stimulation. It should be noted that this mechanism has not been conclusively demonstrated and remains a hypothesis-driven interpretation based on anatomical proximity and sporadic clinical observations. Nevertheless, this structural adjacency is considered a potential anatomical basis for the false-positive signals occasionally encountered during the initial stages of vagal mapping [25].
For a detailed summary of each anatomical variation with its corresponding expected neuromonitoring features and clinical implications, the reader is referred to Table 1.
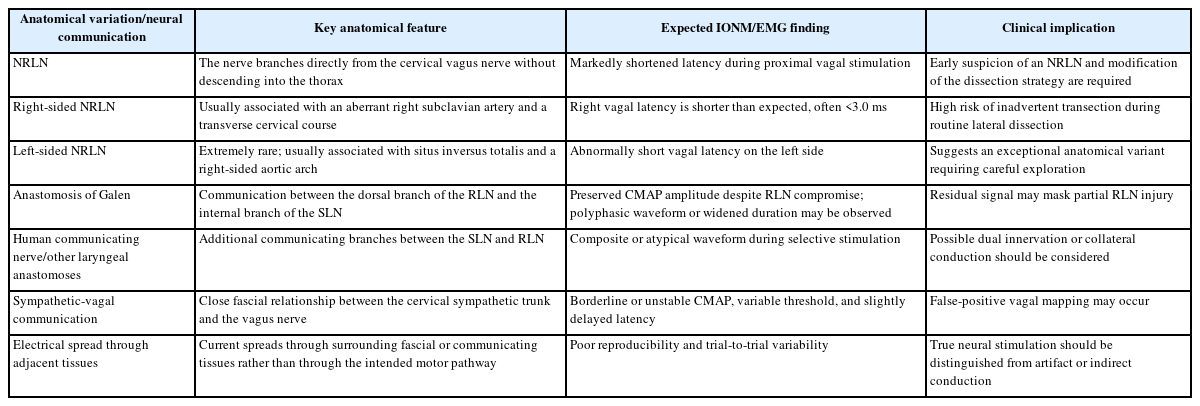
Major anatomical variations and neural communications relevant to thyroid and parathyroid surgery and their expected IONM features
Electrophysiological Signatures of Anomalous Innervation
Identifying these anatomical variations intraoperatively relies on evaluating multiple parameters of the evoked CMAP beyond simple amplitude thresholds, including latency, waveform morphology, and stimulation thresholds (Figure 2).
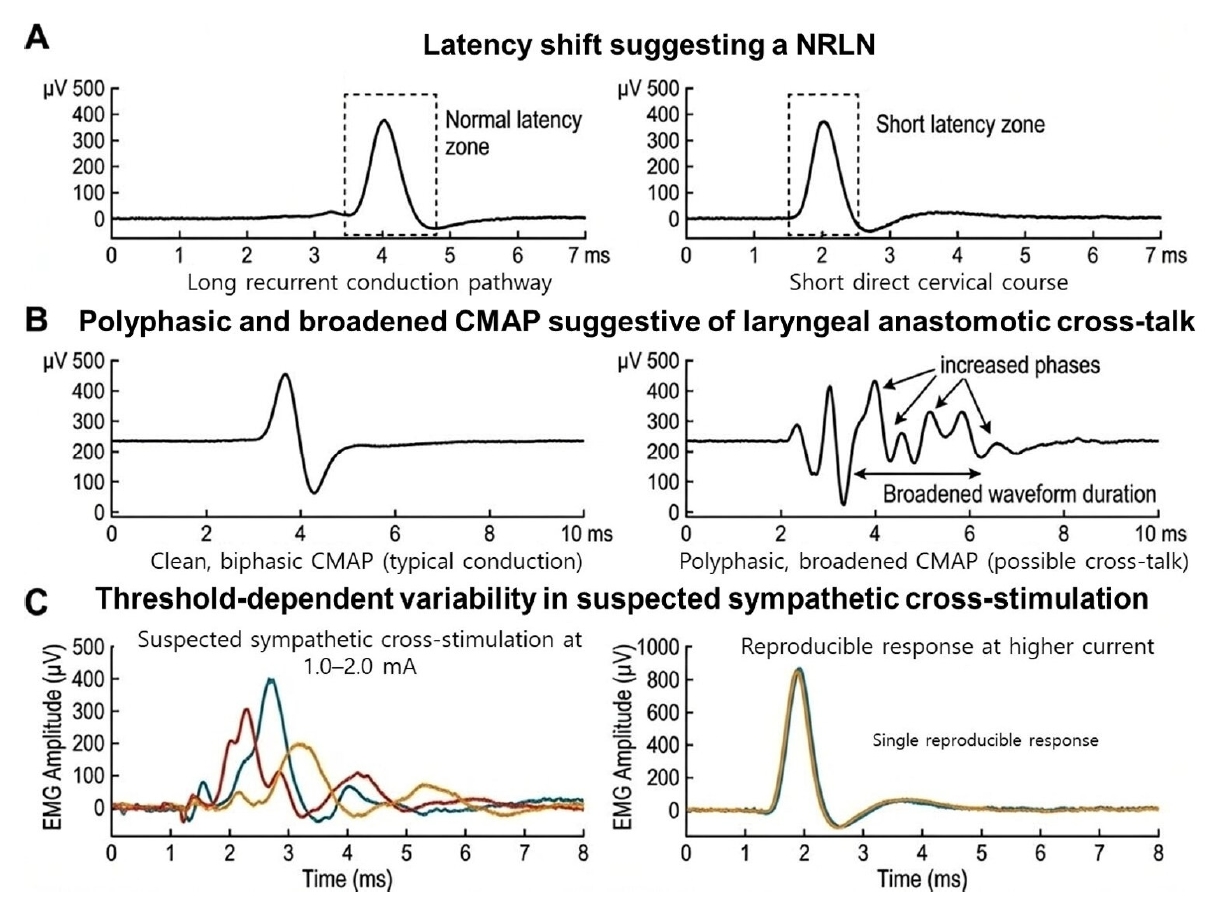
Representative electrophysiological signatures of anomalous innervation during intraoperative neuromonitoring. (A) A shortened latency during proximal vagal stimulation suggests a NRLN, reflecting the shorter direct cervical conduction course compared with the normal RLN. (B) Polyphasic and broadened CMAP waveforms are suggestive of possible laryngeal anastomotic cross-talk. In this setting, the CMAP may remain detectable despite RLN compromise, while showing increased phases and prolonged waveform duration. (C) Threshold-dependent variability in suspected sympathetic cross-stimulation. Variable responses at lower stimulation currents may suggest false-positive mapping, whereas a reproducible response at higher current may indicate current-dependent signal stabilization. NRLN, non-recurrent laryngeal nerve; RLN, recurrent laryngeal nerve; CMAP, compound muscle action potential; EMG, electromyography; ms, milliseconds.
1. Latency shifts as a marker for the non-recurrent laryngeal nerve
For the NRLN, a notably reduced latency during proximal vagal stimulation (identified during the V1 or V2 steps of the INMSG protocol) is recognized as a key electrophysiological feature [27,28]. The recorded latency measures the time required for the electrical impulse to travel from the stimulation probe to the recording electrodes on the endotracheal tube. Because the conduction velocity of myelinated somatic motor fibers is relatively constant, this latency is directly proportional to the anatomical distance the impulse travels [27].
In a typical anatomical configuration, the action potential must travel down into the thorax and ascend back through the tracheoesophageal groove. Normative clinical databases establish that the standard right vagal latency generally ranges from 3.5 to 5.5 milliseconds (ms) [27,29]. When an NRLN is present, it branches directly from the cervical vagus, abruptly shortening the physical conduction distance. Consequently, the electrophysiological signature of an NRLN is a distinctly short vagal latency, frequently observed between 1.5 and 2.5 ms [29]. Clinical studies indicate that a right vagal latency of consistently less than 3.0 ms raises the clinical suspicion of an NRLN, prompting necessary changes in surgical strategy.
2. Waveform morphology and anastomotic cross-talk
Neuronal cross-talk, such as that potentially facilitated by the anastomosis of Galen, presents different signal characteristics [9]. When dual innervation is functionally present, the CMAP recorded at the vocalis muscle is a composite summation of action potentials arriving from both the RLN and SLN pathways [30].
If the RLN experiences a proximal conduction block due to traction or mechanical compression, it has been postulated that the SLN might act as a compensatory motor conduit, although this pathway has not been conclusively validated in controlled clinical settings [31]. The resulting electrophysiological signature is an altered CMAP that may maintain a baseline amplitude (often remaining above the standard 100 μV threshold) despite RLN compromise. The literature notes that these compensatory waveforms often exhibit structural changes, such as increased polyphasia (multiple peaks within a single waveform) and widened durations. This morphological distortion is hypothesized to reflect the asynchronous arrival of motor units through parallel pathways of varying resistance and length, though definitive electrophysiological demonstration of this mechanism in a surgical context remains limited [32,33]. Therefore, observation of waveform morphology and the area under the curve is suggested as a valuable adjunct when evaluating potential neural cross-talk [34].
3. Threshold dynamics in sympathetic cross-stimulation
Distinguishing true vagal signals from sympathetic-vagal cross-stimulation artifacts generally involves assessing stimulation thresholds and signal stability [26]. The sympathetic trunk is functionally and histologically distinct from the somatic motor fibers of the vagus nerve. Due to differences in fiber myelination and surrounding connective tissue impedance, the sympathetic trunk typically requires a higher electrical stimulation current to elicit a propagated response that mimics a vagal signal at the vocal folds [26,35].
Clinical observations suggest that potential sympathetic cross-talk may produce a CMAP characterized by significant trial-to-trial amplitude variability (unstable signals) and a slightly delayed latency compared to true vagal stimulation [36]. This delay may plausibly occur because the electrical impulse must bridge higher-resistance communicating tissues or fascial planes before entering the vagal motor pathways, although the precise biophysical basis for this observation has not yet been fully characterized. Recognizing these threshold requirements and observing the overall stability of the waveform can assist surgeons in distinguishing between the intended neural target and surrounding autonomic structures [26].
Clinical Troubleshooting and Surgical Strategies
Based on the anatomical and electrophysiological principles outlined above, several troubleshooting strategies have been proposed to navigate atypical IONM signals within the standard four-step procedure (V1-R1-R2-V2), as summarized in Table 2.
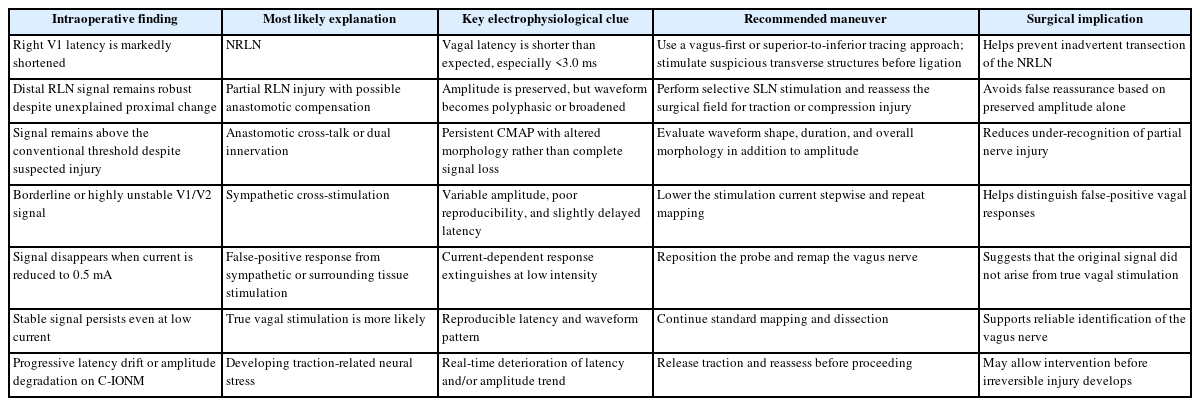
Practical troubleshooting strategies for atypical IONM findings during thyroid and parathyroid surgery
1. Navigating the non-recurrent laryngeal nerve
When evaluating the surgical field, the initial vagal stimulation (V1), performed prior to any central thyroid dissection, serves as an essential screening step. If the right V1 latency is calculated at less than 3.0 ms, various clinical reports recommend modifying the standard lateral-to-medial mobilization of the thyroid lobe [37].
In such scenarios, adopting a "vagus-first" or superior-to-inferior tracing technique has been proposed. This involves meticulously tracing the vagus nerve superiorly along the carotid sheath to visually locate the exact transverse branching point of the NRLN [37]. This preemptive identification strategy is designed to minimize the risk of inadvertent nerve transection. Furthermore, any transverse structure resembling a blood vessel in the middle or upper pole region must be stimulated with the probe prior to ligation to confirm it is not an NRLN [38].
2. Managing anastomotic cross-talk
When managing suspected anastomotic cross-talk during thyroid dissection, selective mapping is considered useful. A challenging clinical scenario involves an unexplained decrease in the proximal RLN amplitude (R2) without a complete loss of signal, while the distal stimulation (R1) remains robust [31,39].
Rather than simply increasing the stimulation current on the RLN in an attempt to artificially recover the signal, targeted stimulation of the SLN external branch at varying intensities can be performed. Observing changes in CMAP polyphasia and amplitude during selective SLN stimulation can help deduce whether the residual signal recorded at the vocalis muscle is bypassing a partial proximal RLN lesion via an anastomosis [31]. Recognizing this phenomenon may prevent false reassurance that the RLN is entirely intact, prompting a careful re-examination of the surgical field for subtle stretch injuries [32].
3. Differentiating sympathetic cross-stimulation
For suspected sympathetic-vagal cross-stimulation during the initial V1 or final V2 mapping stages, current manipulation based on tissue impedance differences can be diagnostic [26]. The sympathetic trunk is typically enveloped in a distinct, higher-resistance prevertebral fascial layer compared to the vagus nerve. Therefore, lowering the stimulation current on the probe can help differentiate the neural source.
For instance, a borderline or highly variable CMAP might be obtained during V1 mapping at standard currents (e.g., 1.0 to 2.0 mA). In this situation, a practical maneuver is to systematically lower the stimulation current to 0.5 mA. If the CMAP entirely extinguishes at the lower current setting, this suggests the signal may represent a false positive potentially originating from the sympathetic trunk. Conversely, if a stable CMAP persists even at 0.5 mA, it more reliably confirms true vagal nerve localization.
Additionally, the utilization of C-IONM via vagal electrodes provides a real-time baseline of latency and amplitude. Observing sudden latency drifts or progressive amplitude degradation in real-time allows for the early detection of traction-induced changes. This early detection provides an opportunity to release tissue tension before permanent structural damage or cross-talk compensation mechanisms are fully triggered.
Conclusion
Anatomical variations and neuronal cross-talk—including the distinct trajectory of the NRLN, the in ternal communications of the anastomosis of Galen, and sympathetic-vagal fascial connections—can influence the signals obtained during IONM. While IONM remains an established tool in modern head and neck surgery, relying solely on basic visual assessments or single amplitude thresholds may occasionally be insufficient when atypical anatomical features are present.
Current literature supports evaluating multiple electrophysiological parameters beyond mere signal presence or absence. Recognizing a shortened vagal latency as an indicator of an NRLN, analyzing waveform morphology for anastomotic compensation, and utilizing threshold dynamics to identify sympathetic cross-talk are practical strategies that enhance intraoperative decision-making. Ultimately, a thorough understanding of these specific electrophysiological signatures remains essential for safe, nerve-sparing surgical practice.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
All work was done by YSK.