First-side loss of signal during planned bilateral thyroidectomy: troubleshooting and intraoperative decision-making
Article information

Abstract
Recurrent laryngeal nerve (RLN) injury is a serious complication of thyroid surgery. Intraoperative neural monitoring allows functional assessment of the RLN during dissection, but first-side loss of signal (LOS) during planned bilateral thyroidectomy creates a difficult intraoperative dilemma. Misinterpreting false LOS may lead to unnecessary staged procedures, while overlooking true LOS risks bilateral vocal fold paralysis. This structured narrative review, based on a focused PubMed search (2000-2026), addresses the practical management of first-side LOS in three steps. First, when LOS occurs, the surgeon must systematically exclude false causes such as equipment failure, endotracheal tube malposition, and residual neuromuscular blockade before accepting LOS as genuine. Second, once confirmed, the injury mechanism (traction versus structural), signal loss pattern (segmental versus global), and any intraoperative recovery on continuous monitoring help estimate the likelihood of postoperative vocal fold palsy. Third, in benign bilateral disease, current evidence generally supports staged thyroidectomy as the safest default to avoid bilateral RLN dysfunction. Immediate contralateral completion may still be considered in high-priority situations such as invasive thyroid cancer or impending airway compromise, following individualized risk-benefit assessment. First-side LOS should be treated as a structured decision point, and standardized troubleshooting combined with careful interpretation of monitoring data can support safer and more transparent surgical judgment.
Introduction
Recurrent laryngeal nerve (RLN) injury remains one of the most feared complications of thyroid surgery because of its impact on phonation, swallowing, airway protection, and overall quality of life. Although visual nerve identification remains the cornerstone of safe thyroidectomy [1,2], intraoperative neural monitoring (IONM) has become an important adjunct because it adds functional assessment of the RLN and vagus nerve during dissection [3,4]. Among all intraoperative monitoring events, loss of signal (LOS) is the most consequential because it may reflect either true neural dysfunction or a reversible technical problem. This distinction becomes especially important during planned bilateral thyroidectomy. If first-side LOS is misinterpreted as true RLN injury, the surgeon may unnecessarily convert a single-stage operation into a staged procedure. Conversely, if true LOS is overlooked and contralateral dissection is continued, the patient may be exposed to the risk of bilateral vocal fold paralysis, a rare but potentially life-threatening complication [5,6].
For this reason, first-side LOS is no longer simply a technical issue related to monitoring quality. It has become a key intraoperative decision point that may alter the extent and sequencing of surgery. International guideline statements have emphasized the importance of standardized monitoring procedures, structured confirmation of LOS, and a cautious operative strategy when true LOS is detected during planned bilateral surgery [4,6]. However, contemporary practice remains heterogeneous. Recent survey data indicate that surgeons still vary substantially in how they interpret LOS, in the confidence they place in signal recovery, and in the conditions under which they would continue contralateral surgery despite first-side signal loss [7]. Similarly, recent evidence synthesis suggests that outcomes after immediate completion thyroidectomy in the setting of first-side LOS remain difficult to interpret because the available studies are heterogeneous in design, indication, monitoring protocol, and endpoint definition [8].
The clinical challenge arises from the fact that LOS is not a uniform event. Apparent LOS may result from recording failure, unstable endotracheal tube contact, equipment-related malfunction, or anesthetic factors rather than from structural or functional nerve injury. Even when LOS is genuine, its implications depend on the likely mechanism of insult, the pattern of signal loss, the degree of intraoperative recovery, and the indication for surgery. In patients undergoing planned bilateral thyroidectomy for benign bilateral disease, confirmed true first-side LOS generally favors a staged strategy to reduce the risk of bilateral RLN dysfunction [6,9]. By contrast, in selected high-priority situations—particularly invasive thyroid cancer, preoperative vocal fold paralysis, or disease threatening the airway or esophagus—contralateral completion may still be considered after individualized risk-benefit assessment [10].
Many existing discussions of LOS are embedded within broader reviews of IONM, RLN injury, or thyroidectomy technique. By contrast, the present review focuses specifically on first-side LOS as a practical decision problem. Three questions are emphasized: How should first-side LOS be confirmed and false LOS excluded? What intraoperative findings help interpret confirmed LOS? When should contralateral surgery be continued, modified, or staged? By addressing these questions, this structured narrative review aims to provide a concise and clinically useful framework for surgeons dealing with first-side LOS during contemporary bilateral thyroid surgery.
Literature Search and Scope
This structured narrative review was based on a focused PubMed search of English-language articles published from January 1, 2000, through March 26, 2026. The search was performed on March 26, 2026. Search terms included combinations of "thyroidectomy," "thyroid surgery," "intraoperative neural monitoring," "loss of signal," "recurrent laryngeal nerve," "staged thyroidectomy," "contralateral surgery," "troubleshooting," and "continuous intraoperative neuromonitoring." Guideline papers, consensus statements, original studies, systematic reviews, and major review articles relevant to LOS during thyroid or parathyroid surgery were considered. Articles dealing exclusively with remote-access thyroidectomy, monitoring of the external branch of the superior laryngeal nerve, isolated anatomical issues, unrelated postoperative voice outcomes, or single case reports were excluded. Additional relevant studies were identified through manual review of the reference lists of key articles. Because this was a structured narrative review rather than a formal systematic review, studies were selected according to predefined thematic relevance to LOS confirmation, false versus true LOS, mechanisms of RLN injury, signal recovery, and intraoperative decision-making after first-side LOS during planned bilateral thyroidectomy.
Confirming First-Side Loss of Signal: Definition, Standardization, and Troubleshooting
When LOS occurs on the first side of a planned bilateral thyroidectomy, the immediate priority is confirmation rather than immediate change in operative strategy. This principle is fundamental because the reliability of all downstream decisions depends on whether the event truly reflects loss of RLN function. According to international standards, LOS generally refers to disappearance or marked reduction of a previously satisfactory electromyographic response after stimulation of the vagus nerve or RLN under appropriate monitoring conditions; in many standardized protocols, a final response of less than 100 µV is considered consistent with LOS [4]. In practical surgery, however, LOS should not be treated as a diagnosis in itself. It is a monitoring finding that must be interpreted in light of baseline signal adequacy, standardized stimulation sequence, recording quality, and the surgical maneuver associated with the event. For that reason, clear documentation of the V1-R1-R2-V2 sequence remains valuable: it provides the framework needed to judge whether a signal change is clinically meaningful, reproducible, and likely to represent true nerve dysfunction [4,6].
A major reason for caution is that the predictive performance of IONM is asymmetrical. A preserved final signal is generally highly reassuring, and the negative predictive value for normal postoperative vocal fold function is consistently high in the literature, often exceeding 95% [4,11]. By contrast, the positive predictive value of LOS for postoperative vocal fold palsy is substantially lower and more variable because LOS may reflect false signal loss, transient neuropraxia, or reversible technical problems rather than lasting RLN dysfunction [4,6,8,11,12]. This asymmetry explains why an intact final signal is reassuring whereas a lost signal cannot be interpreted uncritically. In practical terms, LOS is a warning sign that requires verification, not an automatic declaration of permanent nerve injury.
In most cases, false LOS originates not from interruption of nerve conduction but from failure somewhere along the monitoring chain. Stable IONM requires a functioning monitor, intact stimulating probe and cables, appropriate grounding, preserved neuromuscular transmission, and a reliable recording interface. With standard endotracheal tube-based monitoring systems, the recording interface is especially vulnerable. Neck extension, tracheal rotation, thyroid lobe traction, and repeated laryngeal manipulation can change the relationship between the endotracheal tube electrodes and the true vocal folds, producing abrupt signal disappearance despite preserved neural integrity [13,14]. Recent studies have reinforced this point. Device comparison data suggest that false LOS can be influenced by the recording platform itself [15], and more detailed analysis of endotracheal tube electrodes indicates that recorded amplitudes may differ substantially according to electrode orientation and laterality [16]. These findings support a practical message that is highly relevant to first-side LOS: a missing signal often reflects recording failure rather than true nerve injury.
For similar reasons, alternative recording strategies have been proposed. Thyroid cartilage electrodes may reduce signal instability related to tube displacement and can serve as a useful adjunct in selected settings [17]. Likewise, handheld or nontraditional recording interfaces have been explored as ways to decrease tube-related artifact [15]. At present, however, these approaches should be viewed as promising adjuncts rather than universal standards. Their main importance in the context of this review is conceptual: they demonstrate that the limitations of surface electrode recording are real and that interpretation of LOS must always take recording vulnerability into account.
Technical troubleshooting must therefore begin immediately and systematically. Equipment-related failure is a frequent and often overlooked cause of false LOS. Disconnected leads, probe malfunction, unstable connectors, grounding problems, or console-related issues may all produce absent or inconsistent responses. If LOS is treated reflexively as a nerve event, these correctable causes may be missed. Expert-based troubleshooting recommendations emphasize a stepwise approach: pause the operation, release traction, inspect the monitor and stimulation probe, verify cable continuity and grounding, reassess the recording interface, and then repeat vagus nerve and RLN stimulation once any suspected technical problem has been corrected [18]. This process is not a mere technical ritual. In the setting of planned bilateral thyroidectomy, it is a patient safety measure because it reduces the chance of converting an intended one-stage operation into an unnecessary staged procedure on the basis of artifactual LOS.
Anesthetic factors must be considered with equal seriousness. Electromyographic monitoring depends on sufficient preservation of neuromuscular transmission, and excessive residual neuromuscular blockade may attenuate or abolish the laryngeal response despite preserved RLN function. Unrecognized additional dosing of muscle relaxants, incomplete reversal, or other anesthetic changes may therefore mimic true LOS. Recent work on precision neuromuscular blockade management in thyroid surgery underscores that signal quality depends not only on the surgeon’s handling of the nerve but also on coordinated anesthetic management [19]. Accordingly, suspected LOS should prompt immediate communication with the anesthesiology team regarding recent drug administration, reversal status, and any events that may have altered monitoring reliability. The eventual continue-versus-stage decision is only as trustworthy as the confidence that the observed signal truly reflects nerve status rather than pharmacologic suppression.
From a practical perspective, confirmation of first-side LOS follows a straightforward logic. Dissection is paused and traction released. Baseline monitoring adequacy is verified. The surgeon then checks the equipment, the recording interface, and anesthetic conditions, followed by repeated stimulation of both the vagus nerve and the exposed RLN. If the signal returns after correction of technical or anesthetic factors and remains reproducible, false LOS is likely and contralateral surgery may proceed if otherwise indicated. If the signal remains absent despite structured troubleshooting, true LOS becomes much more likely and the surgeon must move from troubleshooting to interpretation and decision-making. The major causes of first-side LOS and their practical verification steps are summarized in Table 1. A practical management pathway based on this principle is illustrated in Figure 1.
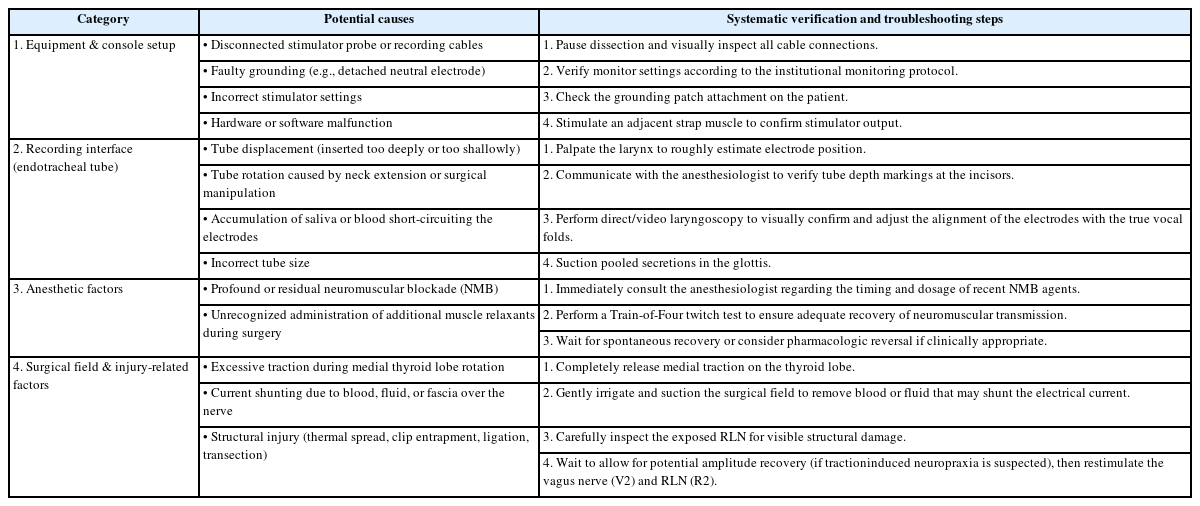
Causes of first-side loss of signal and systematic troubleshooting steps
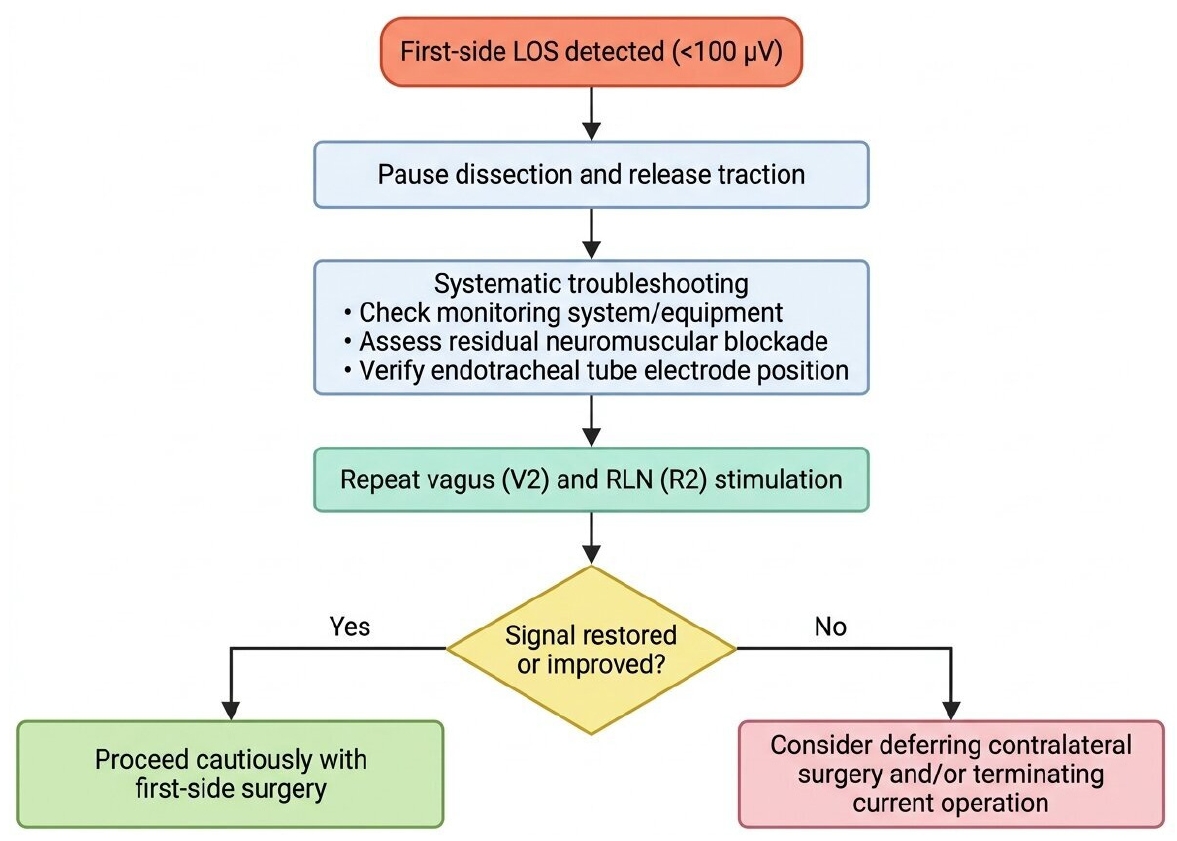
Suggested management algorithm for first-side loss of signal during thyroid surgery. After first-side LOS, dissection should be paused and traction released, followed by systematic troubleshooting and repeat stimulation of the vagus nerve (V2) and RLN (R2). If the signal is restored or improved, surgery may proceed cautiously on the first side. If LOS persists, contralateral surgery may be deferred and a staged approach considered according to the clinical situation. LOS, loss of signal; RLN, recurrent laryngeal nerve.
Interpreting Confirmed Loss of Signal: Mechanism, Pattern, and Recovery
Once false LOS has been reasonably excluded, the next task is to interpret what confirmed LOS is likely to mean. True LOS is a functional sign of RLN stress or injury, but its clinical significance varies according to mechanism, pattern, and reversibility. Mechanistic studies have shown that traction is the most common cause of RLN dysfunction during thyroidectomy, especially during medial thyroid lobe rotation and dissection near the Berry ligament [20,21]. This point is clinically important because traction-related neuropraxia may initially be reversible, whereas thermal injury, ligation, clip entrapment, or transection generally imply a higher probability of structural damage and persistent dysfunction [22]. Mechanism does not determine postoperative outcome with certainty, but it provides essential context for real-time risk interpretation after first-side LOS.
Further refinement is provided by the distinction between segmental and global LOS. In some patients, systematic RLN mapping reveals a discrete lesion point along the exposed nerve, suggesting focal injury such as thermal spread, compression, ligation, or clip-related trauma. This pattern is typically described as segmental LOS. In others, no focal lesion point can be identified and signal loss appears diffuse, a pattern more compatible with generalized traction-related dysfunction or proximal impairment; this is referred to as global LOS [23]. Although this distinction is not an absolute predictor of postoperative vocal fold movement, it is clinically useful. Segmental LOS tends to raise greater concern for localized structural injury, whereas global LOS may fit better with a neuropraxic mechanism and possible intraoperative recovery. Just as importantly, the classification encourages more precise documentation of the event and facilitates better communication within the operative team.
Continuous IONM (cIONM) has added another layer of interpretive value. In contrast to intermittent stimulation, cIONM may reveal progressive amplitude decline and latency changes before complete LOS develops, thereby identifying evolving nerve stress and creating an opportunity to release traction before full neuropraxia occurs [24]. A commonly used warning pattern is a combined event characterized by a greater than 50% decrease in amplitude together with a greater than 10% increase in latency; when these changes persist or progress, the risk of complete LOS increases substantially [12,24]. This feature is especially relevant for difficult bilateral thyroidectomy, where early recognition of impending injury may prevent first-side complete LOS altogether. Even after LOS occurs, cIONM and repeated stimulation can help clarify whether any signal recovery occurs after cessation of the suspected insult. Schneider et al. [25] showed that the dynamics of signal loss and recovery correlate with early postoperative vocal fold function, suggesting that recovery carries useful prognostic information. However, this information should be interpreted cautiously. Recovery of the electromyographic signal does not guarantee normal postoperative motion, and persistent LOS does not inevitably imply permanent palsy. Therefore, cIONM and signal recovery should be regarded as tools for risk stratification rather than definitive determinants of surgical strategy.
Decision-Making After First-Side True Loss of Signal: Continue or Stage?
After first-side LOS has been confirmed as genuine, the surgeon reaches the central decision point of this review: should the planned bilateral operation proceed, be modified, or be converted to a staged procedure? This decision cannot be based on electrophysiologic data alone. Rather, it must integrate the reliability of LOS confirmation, the likely severity of the first-side neural insult, the indication for surgery, the urgency of disease control, and the potential consequences of bilateral RLN dysfunction. In this setting, IONM does not function as an absolute rule generator; instead, it serves as a structured decision-support tool.
In patients undergoing planned bilateral thyroidectomy for benign bilateral disease, the dominant principle is precaution. Once true LOS has been confirmed on the first side, staged thyroidectomy is generally the preferred strategy because it reduces the risk of bilateral vocal fold paralysis [4,6]. The rationale is practical and compelling. Although many unilateral RLN dysfunctions are transient and clinically manageable, bilateral RLN dysfunction may cause severe airway compromise and may require urgent airway intervention. At the time LOS occurs, the surgeon cannot reliably know which patient will recover rapidly and which patient will not. Therefore, in an otherwise elective benign setting, many guideline-based approaches accept the inconvenience, additional cost, and psychological burden of a second operation as preferable to the possibility of bilateral vocal fold paralysis [4,6,9].
Available clinical studies broadly support this risk-avoidance framework, even though the evidence is not uniform in methodology or endpoint definition. Sitges-Serra et al. [23] prospectively evaluated LOS on the first side during total thyroidectomy and demonstrated its direct impact on surgical strategy. Calò et al. [26] further addressed whether two-staged thyroidectomy is justified and supported a cautious approach in selected bilateral benign cases. More recently, survey data from the International Neural Monitoring Study Group (INMSG) showed that management of first-side LOS remains variable among surgeons, indicating that although the principle of staged surgery is widely recognized, real-world application is still influenced by individual practice patterns and local risk tolerance [7]. Likewise, the systematic review and meta-analysis by Ramesh et al. [8] underscores that evidence regarding immediate total thyroidectomy after first-side LOS remains heterogeneous. Together, these observations suggest that staged thyroidectomy in benign bilateral disease is not a rule supported by perfect predictive certainty, but it remains the most defensible default strategy after confirmed true LOS.
The decision, however, is not purely biomedical. Staged surgery introduces a second episode of anticipatory anxiety, a second general anesthetic exposure, additional direct and indirect costs, and potential delay in completing treatment. It may also increase time away from work and create uncertainty for patients who expected definitive surgery in a single session. These patient-centered burdens should not be minimized; indeed, they help explain why some surgeons remain reluctant to stage surgery after LOS [27]. Nevertheless, these disadvantages must be weighed against the potential severity of bilateral vocal fold paralysis. In most elective benign bilateral cases, the balance still favors staging, but this conclusion should be communicated as a patient-centered trade-off rather than as a purely technical recommendation.
Several factors strengthen the argument for staging. These include bilateral multinodular goiter, Graves disease without urgent compressive symptoms, and other benign conditions in which delayed completion is feasible without substantial oncologic or functional disadvantage [28,29]. Persistent LOS despite full troubleshooting, absent or minimal signal recovery, and a mechanism strongly suggestive of structural injury all increase concern and further favor stopping after the first side. In addition, staged surgery becomes easier to implement when the possibility has been discussed preoperatively. Patients scheduled for bilateral thyroidectomy should ideally be informed that surgery may be intentionally divided into two stages if true LOS occurs. This preoperative discussion is not simply a medicolegal precaution; it is part of shared decision-making and helps align intraoperative safety choices with patient expectations.
At the same time, the principle of staging should not be applied rigidly in every case. The clearest and most important exception is invasive thyroid cancer. In patients with gross extrathyroidal extension, preoperative vocal fold paralysis, significant tumor burden, or disease threatening the airway or esophagus, the consequences of incomplete surgery may be substantial. The 2018 INMSG guideline on RLN management in invasive thyroid cancer emphasizes that oncologic necessity may justify continued resection even when monitoring findings are concerning [10]. In such cases, the key question is not whether staging is generally safer—it usually is—but whether stopping the operation would produce greater overall harm. If delay is likely to compromise resectability, oncologic completeness, or control of airway-related disease, immediate contralateral completion may be justified. However, such decisions should remain exceptional and should preferably be made by surgeons experienced in both advanced thyroid cancer and the interpretive limits of IONM.
Importantly, justified continuation should be distinguished from optimistic continuation. Proceeding to the second side should not be based merely on hope that first-side LOS will prove transient or that postoperative vocal fold motion will eventually recover. Interventions proposed to improve signal recovery, such as steroid administration after LOS, are interesting and may merit further study, but they do not currently redefine the standard operative approach [30]. Likewise, partial intraoperative signal recovery may somewhat reduce concern, but it should not override the broader clinical context. A surgeon who elects to continue despite confirmed true LOS should be able to articulate clearly why the benefit of immediate completion outweighs the risk of bilateral dysfunction. The major clinical factors favoring staged thyroidectomy versus immediate contralateral completion are summarized in Table 2.
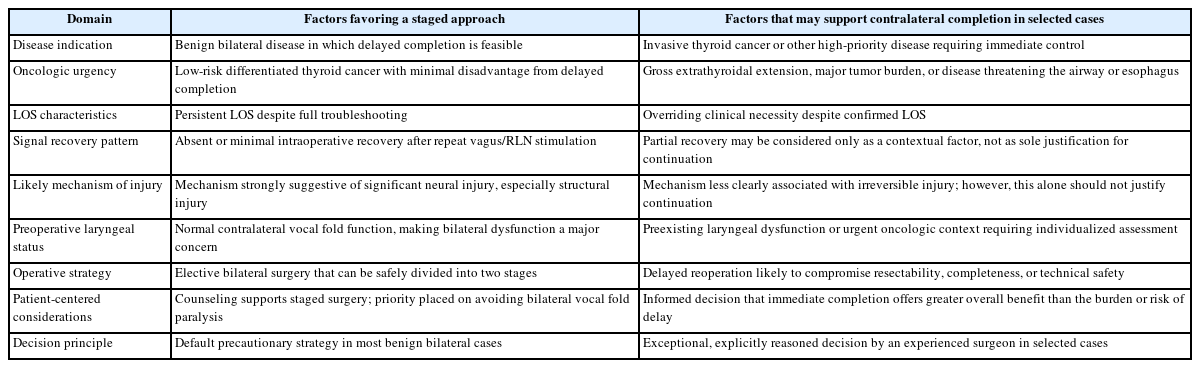
Factors to consider when deciding whether to stage or continue surgery after confirmed first-side true LOS
Practical Implications, Limitations, and Conclusions
Several practical implications follow from this framework. First, patients undergoing planned bilateral thyroidectomy should be counseled preoperatively that surgery may be intentionally staged if first-side true LOS occurs. Second, LOS management should be treated as a team-based process involving the surgeon and anesthesiologist, particularly when recording interface issues or neuromuscular blockade may affect interpretation. Third, postoperative laryngoscopic evaluation remains essential after LOS, both to correlate intraoperative findings with actual vocal fold function and to guide planning for completion surgery if staging is chosen. Fourth, the LOS event should be documented in a structured manner, including baseline monitoring values, troubleshooting steps, vagus and RLN stimulation findings, suspected mechanism, recovery pattern, and the rationale for the final operative decision.
The timing of completion surgery after staged thyroidectomy should be guided primarily by postoperative laryngeal assessment and the clinical priority of the residual contralateral disease. In most benign cases, early postoperative laryngoscopy is appropriate to establish whether ipsilateral vocal fold motion is preserved, recovering, or persistently impaired. If vocal fold motion recovers and there is no urgent need for immediate reoperation, completion surgery can be planned electively under more controlled conditions. If paresis persists, management should be individualized.
This review also has limitations that should be acknowledged. The available evidence on first-side LOS is derived largely from guideline statements, retrospective observational studies, expert opinion, survey data, and a limited number of systematic syntheses. Direct comparative evidence for "continue versus stage" strategies remains limited, and study heterogeneity in LOS definition, monitoring protocol, and postoperative endpoint assessment complicates pooled interpretation.
Future work should aim to strengthen the evidence base with prospective multicenter studies using standardized LOS definitions, uniform laryngoscopic follow-up, and clearly reported patient-centered outcomes, including cost, quality of life, and burden of staged surgery. Better integration of cIONM metrics, recovery patterns, and alternative recording technologies may also improve risk stratification and reduce unnecessary staged procedures caused by false LOS.
In conclusion, first-side LOS during planned bilateral thyroidectomy should be regarded as a structured decision point rather than an automatic indication either to stop or to continue surgery. The first task is confirmation: false LOS due to recording, equipment, or anesthetic factors must be excluded before the monitoring finding is allowed to alter operative strategy. Once true LOS is confirmed, interpretation of mechanism, pattern, and signal recovery can refine risk assessment, but in benign bilateral disease the balance of current evidence generally favors staged thyroidectomy to minimize the risk of bilateral vocal fold paralysis. Immediate contralateral completion may still be justified in selected high-priority situations, particularly invasive thyroid cancer, but such decisions should remain individualized and explicitly reasoned.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
All work was done by SJL.