Management of recurrent papillary thyroid carcinoma: diagnosis, surveillance, and treatment strategies
Article information

Abstract
Papillary thyroid carcinoma (PTC) accounts for over 85% of all thyroid malignancies and generally has a favorable prognosis, with 10-year overall survival exceeding 90%. Nonetheless, locoregional recurrence develops in 5%-30% of patients within the first decade following initial treatment, and cervical lymph node metastasis represents the predominant recurrence pattern. Accurate detection relies on serial neck ultrasonography, serum thyroglobulin measurement, fine-needle aspiration cytology with thyroglobulin washout analysis, and selective use of cross-sectional imaging or 18F-fluorodeoxyglucose positron emission tomography/computed tomography. Management should be individualized through a multidisciplinary framework, ranging from active surveillance for small, indolent nodal disease to compartment-oriented surgical reoperation, radioactive iodine therapy, external beam radiation, percutaneous ablation, and systemic targeted therapy for progressive radioactive iodine-refractory disease. This review synthesizes current evidence and guideline recommendations for recurrent PTC. Particular emphasis is placed on the 2015 and 2025 American Thyroid Association guidelines and the National Comprehensive Cancer Network Version 1.2025 guidelines to provide a structured, clinically oriented approach.
Introduction
Papillary thyroid carcinoma (PTC) is the most prevalent histologic subtype of differentiated thyroid cancer (DTC), representing more than 85% of all thyroid malignancies [1]. Most patients with PTC achieve favorable long-term outcomes, with disease-specific mortality rates of less than 5% at 20 years following appropriate initial treatment consisting of thyroidectomy with or without radioactive iodine (RAI) therapy and thyroid-stimulating hormone (TSH) suppressive therapy [1,2]. Despite this perspective, locoregional recurrence develops in approximately 5%-30% of patients within the first 10 years after primary surgery, with most events occurring in the central and lateral cervical lymph node compartments. Reoperative surgery in this setting poses unique challenges owing to scar tissue and disrupted anatomy, which increase the risk of injury to adjacent structures [2,3]. The wide variability in reported recurrence rates reflects differences in initial disease extent, completeness of surgical resection, risk stratification category, and intensity of postoperative surveillance.
The 2015 American Thyroid Association (ATA) guidelines, which remain a foundational reference for DTC management, define disease-free status after initial therapy by the absence of clinical and imaging evidence of tumor and low serum thyroglobulin (Tg) levels, specifically unstimulated Tg less than 0.2 ng/mL or TSH-stimulated Tg less than 1 ng/mL in the absence of interfering anti-thyroglobulin antibodies (TgAb) [2]. The 2025 ATA guidelines, published as a dedicated DTC-specific update, have refined risk stratification and introduced response-adapted surveillance recommendations while maintaining the core management principles of the prior edition [4]. Structural recurrence refers to the appearance of biopsy-proven or radiologically suspicious disease in a patient who previously achieved an excellent response to therapy.
In clinical practice, structurally evident disease detected after initial therapy may represent either persistent disease that was not completely eradicated at the time of primary treatment or true recurrence in a patient who previously achieved remission. While this distinction carries theoretical prognostic implications, the practical diagnostic and therapeutic approach is largely similar and revolves around accurate restaging and multidisciplinary treatment planning.
A substantial proportion of reoperations for PTC occur within the first 2 years after initial surgery, often reflecting persistent rather than truly recurrent disease [3,5]. These findings underscore the importance of close postoperative surveillance, particularly during the early years. This review synthesizes the current evidence to provide a clinically practical framework for diagnosing and managing recurrent PTC. The discussion is guided by the 2015 ATA guidelines [2] as the foundational reference, the 2025 ATA guidelines [4] as the most recent DTC-specific update, and the National Comprehensive Cancer Network (NCCN) Thyroid Carcinoma Version 1.2025 guidelines [6], which place particular emphasis on systemic therapy and molecular testing. A comprehensive overview of the diagnostic and management algorithm for recurrent PTC is presented in Figure 1.
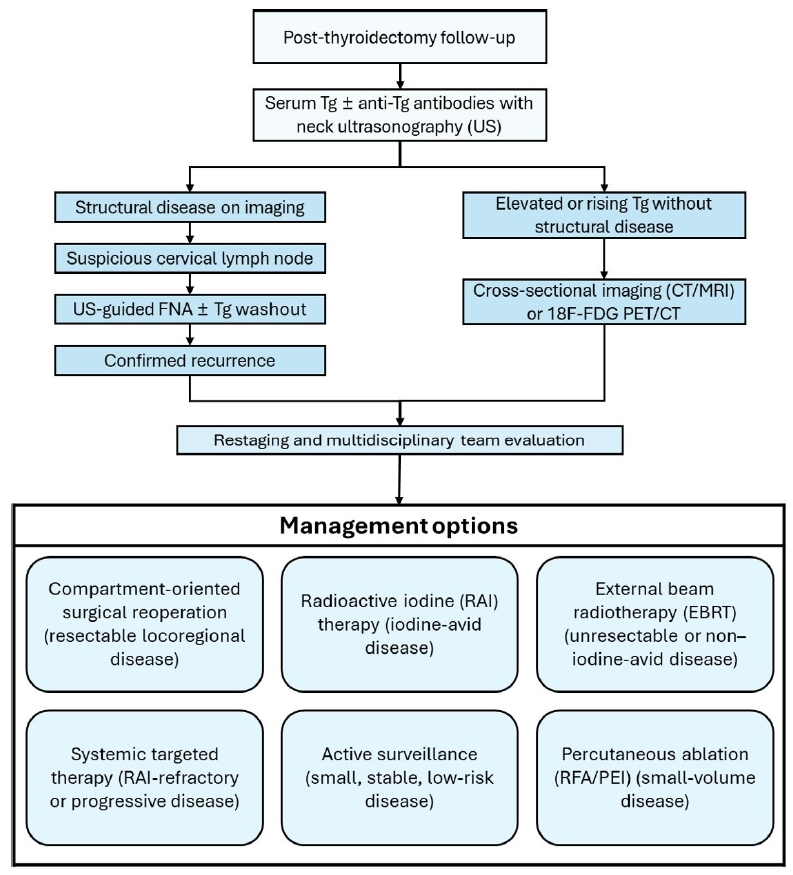
Clinical algorithm for the diagnosis and management of recurrent papillary thyroid carcinoma. Postthyroidectomy follow-up includes serum Tg measurement and neck US. Structural recurrence is confirmed by US-guided FNA with or without Tg washout, while elevated Tg without structural disease warrants additional imaging. Management is individualized and includes surgery, RAI therapy, EBRT, systemic therapy, active surveillance, and percutaneous ablation. Tg, thyroglobulin; FNA, fine-needle aspiration; CT, computed tomography; MRI, magnetic resonance imaging; 18F-FDG PET/CT, 18F-fluorodeoxyglucose positron emission tomography/computed tomography; RFA, radiofrequency ablation; PEI, percutaneous ethanol injection.
Diagnosis of Recurrent Papillary Thyroid Carcinoma
1. Neck ultrasonography
Neck ultrasonography (US) is the primary imaging modality for detecting locoregional recurrence of PTC. It has been reported to achieve high sensitivity for identifying suspicious cervical lymph nodes, approaching 90% in selected series, although performance varies with lesion size, compartment location, operator experience, and history of prior surgery [2,7]. In clinical practice, multiple complementary diagnostic modalities are used for evaluation, as summarized in Table 1. Sonographic features that raise concern for metastatic lymph nodes include loss of the fatty hilum, rounded morphology, cortical hyperechogenicity, cystic change, microcalcifications, and peripheral vascularity on Doppler interrogation [7], as summarized in Table 2. The ATA guidelines recommend periodic neck US at 6- to 12-month intervals during initial follow-up, with the frequency subsequently adjusted based on the patient's risk of recurrence and response to therapy [2,4]. Patients classified as having an excellent response may be followed less frequently, whereas those with indeterminate, biochemically incomplete, or structurally incomplete responses warrant closer surveillance.
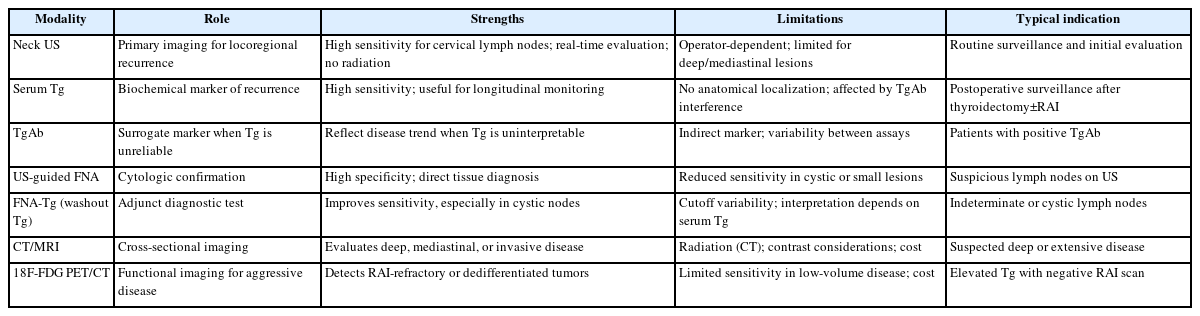
Summary of diagnostic modalities for recurrent papillary thyroid carcinoma
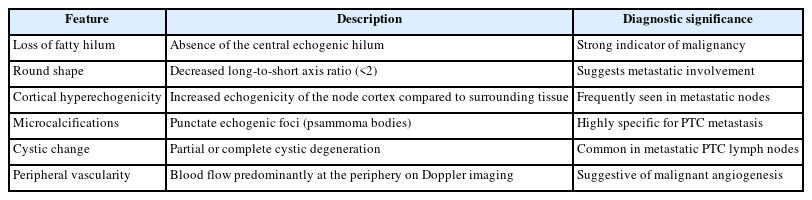
Sonographic features of metastatic cervical lymph nodes in PTC
2. Serum thyroglobulin and anti-thyroglobulin antibodies
Serum Tg serves as a biochemical tumor marker for DTC following total thyroidectomy and RAI ablation. A rising or persistently elevated Tg level, even in the absence of structural disease, may suggest residual or recurrent tumor [2,8]. However, Tg alone lacks spatial resolution. In the postoperative setting after total thyroidectomy and RAI remnant ablation, an unstimulated Tg exceeding approximately 2 ng/mL may suggest structural disease, although the clinical context, including the Tg trend over time, the TSH level at the time of measurement, and the specific Tg assay used, must be carefully considered [8,9]. In general terms, lower Tg values (less than 10 ng/mL) may be more commonly associated with cervical nodal disease, intermediate values (approximately 20-500 ng/mL) with pulmonary metastases, and markedly elevated values with osseous involvement. However, substantial overlap exists among these categories, and these ranges should not be interpreted as definitive thresholds [9].
An important caution is that TgAb are present in up to 25% of patients with DTC and can interfere with immunometric Tg assays, yielding falsely low Tg measurements [8]. In such patients, trending TgAb levels over time may serve as a surrogate tumor marker: declining TgAb concentrations generally correlate with disease remission, whereas rising or persistently elevated TgAb levels may signal recurrence. The combined sensitivity of neck US and serum Tg exceeds that of either modality alone, providing a strong rationale for their concurrent use in routine surveillance [7,9].
3. Fine-needle aspiration cytology and thyroglobulin washout
When neck US identifies a suspicious lymph node, US-guided fine-needle aspiration (FNA) cytology is recommended to confirm the diagnosis before any therapeutic intervention. FNA cytology alone achieves high diagnostic accuracy for solid, overtly suspicious nodes; however, its sensitivity diminishes when the aspirated lymph node contains predominantly cystic fluid, exhibits degenerative changes, or yields a nondiagnostic cytologic specimen [10].
Measurement of Tg in the FNA needle washout fluid (FNA-Tg) substantially enhances diagnostic sensitivity in these settings. The rationale for FNA-Tg measurement is based on the secretion of Tg by metastatic DTC cells within involved lymph nodes, which can be detected in the saline washout of the aspirating needle at concentrations far exceeding serum levels. Reported cutoff values vary widely according to assay, serum Tg status, and institutional protocol; therefore, FNA-Tg should be interpreted in conjunction with cytology, imaging findings, and serum Tg/TgAb status [10,11]. The ATA guidelines endorse the measurement of FNA-Tg for suspicious lymph nodes selected for biopsy during surveillance, particularly when cytology is indeterminate or nondiagnostic [2,4].
When interpreting FNA-Tg results, clinicians should be aware that serum Tg levels may influence washout concentrations, and some authors advocate expressing FNA-Tg relative to the concurrent serum Tg. In patients with elevated TgAb, FNA-Tg results generally remain reliable because TgAb concentrations in the washout fluid are typically negligible compared to those in serum [11]. Beyond its diagnostic role, FNA-Tg mapping of multiple suspicious nodes across different cervical compartments aids in preoperative surgical planning by delineating the anatomic extent of recurrence and guiding compartment-oriented dissection.
4. Cross-sectional imaging and 18F-fluorodeoxyglucose positron emission tomography/computed tomography
Computed tomography (CT) and magnetic resonance imaging of the neck and chest are reserved for cases in which US alone cannot fully characterize the extent of recurrence, particularly when retropharyngeal, mediastinal, or deep lateral compartment disease is suspected [2,6]. When CT is performed for surgical planning, iodinated contrast may be used, provided that RAI therapy, if planned, is deferred for an adequate washout period (typically 4-8 weeks).
18F-Fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) has its principal role in the evaluation of patients with a rising Tg but negative RAI whole-body scan, a clinical scenario that suggests dedifferentiation of tumor cells with loss of iodine avidity and increased glucose metabolism [2,12]. In this context, 18F-FDG PET/CT identifies sites of disease in approximately 60%-80% of patients and also provides prognostic information, as FDG-avid lesions tend to behave more aggressively and respond less favorably to RAI therapy [12]. The ATA and NCCN guidelines recommend 18F-FDG PET/CT for Tg-positive, iodine-negative disease, particularly when the serum Tg exceeds 10 ng/mL [2,4,6].
Management of Recurrent Papillary Thyroid Carcinoma
Management of recurrent PTC should be individualized based on the anatomic location and extent of recurrence, the degree of iodine avidity, the rate of disease progression, patient comorbidities, potential morbidity of the proposed intervention, and patient preferences through shared decision-making, as summarized in Table 3. A multidisciplinary discussion involving endocrinology, head and neck surgery, nuclear medicine, medical oncology, and radiation oncology is essential for complex or multiply recurrent cases.
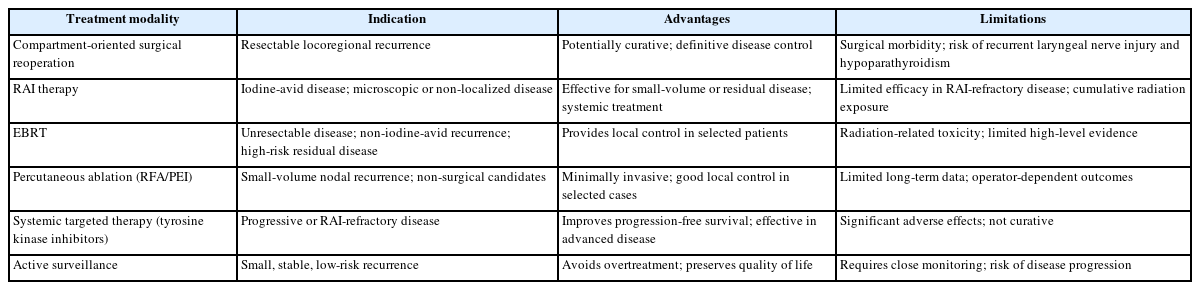
Comparison of management strategies for recurrent papillary thyroid carcinoma
1. Active surveillance
Not every structurally identified recurrence requires immediate intervention. The ATA guidelines acknowledge that active surveillance is a reasonable strategy for small-volume cervical lymph node recurrences, generally nodes measuring less than 8-10 mm in the smallest diameter, that are not in a threatening anatomic location, are not growing, and are not associated with a rapidly rising Tg [2,4]. A prospective observational study by Robenshtok et al. [13] demonstrated that small recurrent lymph nodes (1 cm or less) managed conservatively grew by a median of only 9% over 5 years, and the majority did not require intervention during that period. Active surveillance entails serial US at 6- to 12-month intervals with concurrent Tg measurement. Patients with progressive nodal enlargement, rapidly rising Tg or a Tg doubling time shorter than 1 year, symptomatic disease, lesions adjacent to critical structures, bulky or multiple nodal disease, aggressive histology, or inability to comply with close follow-up are generally unsuitable for observation and should be reconsidered for therapeutic intervention.
2. Surgical management
Compartment-oriented surgical reoperation remains the standard treatment option for appropriately selected patients with resectable locoregional recurrence of PTC. In selected series, first reoperation has been reported to achieve disease-free status, defined as undetectable Tg and no structural evidence of disease, in approximately 50% of patients, although outcomes vary according to tumor burden, prior surgery, disease location, and surgical expertise, and this rate declines with subsequent reoperations [3,14]. Reoperation in the previously dissected neck carries an elevated risk of injury to the recurrent laryngeal nerve (RLN) and the parathyroid glands, with reported rates of permanent hypoparathyroidism up to 5%-10% and permanent vocal cord paralysis up to 2%-5% in experienced centers [14,15]. These risks reinforce the importance of referral to a high-volume thyroid surgeon. Intraoperative neuromonitoring may be considered as an adjunct to enhance nerve identification and functional assessment during revision surgery, with supportive but not yet definitive evidence for reducing RLN injury in the reoperative setting [16,17].
Central compartment re-dissection is a technically challenging situation due to the dense fibrosis from prior surgery and the intimate proximity of the RLNs and parathyroid remnants. Lateral compartment re-dissection, while associated with somewhat less nerve risk, requires careful dissection around the spinal accessory nerve, phrenic nerve, and great vessels. The NCCN Version 1.2025 guidelines recommend compartment-oriented dissection rather than selective removal of individual nodes, as the former approach is associated with lower rates of subsequent re-recurrence [6].
3. Radioactive iodine therapy
RAI therapy serves as an adjunct to surgery for patients with known or suspected residual iodine-avid disease and as a primary modality for non-localizable disease suggested by an elevated Tg without structural correlate on imaging [2,6]. Its role in the postoperative management of recurrent PTC depends on the capacity of the recurrent tumor to concentrate iodine, which can be assessed by diagnostic RAI whole-body scanning. RAI therapy tends to be most effective for small-volume residual disease, pulmonary micrometastases, and iodine-avid nodal disease that is not amenable to surgical resection. The decision to administer RAI must weigh the anticipated benefit against cumulative radiation exposure, particularly in patients who have already received multiple treatments, as the risks of salivary gland dysfunction, bone marrow suppression, and secondary malignancies increase with rising cumulative administered activity [2].
4. External beam radiation therapy
External beam radiation therapy (EBRT) is not a standard first-line approach for recurrent PTC but may be considered in specific clinical situations: unresectable disease with gross residual tumor threatening the airway or other critical structures, non-iodine-avid locoregional recurrence that is not amenable to surgery or RAI, and as an adjuvant treatment following resection of recurrence with microscopic positive margins in the setting of aggressive histopathologic variants [2,6]. The evidence supporting EBRT in DTC remains limited to retrospective series, and its use should be carefully weighed against the risks of radiation-associated fibrosis, dysphagia, and damage to adjacent structures.
5. Percutaneous ablation techniques
US-guided percutaneous ethanol injection (PEI) and radiofrequency ablation (RFA) have emerged as minimally invasive alternatives for treating small-volume cervical lymph node recurrences in patients who are poor surgical candidates, who decline reoperation, or who have limited disease amenable to focal therapy. Published series have reported favorable volume reduction and Tg responses for carefully selected small nodal recurrences treated with RFA or PEI, although these outcomes may vary according to lesion size, location, operator experience, and follow-up duration [18,19]. These techniques may also serve as a bridge to other therapies in patients with comorbidities that temporarily preclude surgery [2].
6. Systemic targeted therapy for radioactive iodine-refractory disease
Although the present review focuses on PTC, systemic therapy data are often derived from broader RAI-refractory DTC (RR-DTC) populations that include PTC as the predominant histologic subtype. Approximately 5%-15% of patients with recurrent DTC ultimately develop RR-DTC, defined by the ATA guidelines as the absence of RAI uptake in known structural lesions, disease progression despite RAI therapy within 12 months, or persistence of disease after a cumulative RAI activity exceeding 600 mCi [2]. The availability of systemic targeted therapies has expanded treatment options for these patients.
Two multi-kinase inhibitors have been approved for RR-DTC on the basis of phase III trials. Lenvatinib, evaluated in the SELECT trial, demonstrated a median progression-free survival (PFS) of 18.3 months versus 3.6 months with placebo, with an objective response rate of approximately 64.8% [20]. Sorafenib, evaluated in the DECISION trial, demonstrated a median PFS of 10.8 months versus 5.8 months with placebo and an objective response rate of approximately 12.2% [21]. Both agents carry significant toxicity profiles, including hypertension, diarrhea, palmar-plantar erythrodysesthesia, and fatigue for lenvatinib, and similar dermatologic and gastrointestinal toxicities for sorafenib, necessitating close monitoring and proactive dose modification.
Beyond multi-kinase inhibitors, the identification of actionable molecular alterations has broadened the therapeutic armamentarium. In patients harboring RET fusions or mutations, the highly selective RET inhibitors selpercatinib and pralsetinib have demonstrated durable responses [22,23]. For the rare subset of PTC driven by NTRK gene fusions, the tropomyosin receptor kinase (TRK) inhibitors larotrectinib and entrectinib offer histology-agnostic antitumor activity with favorable response rates and a manageable safety profile [24,25]. In BRAF V600E-mutated cases, which constitute a substantial proportion of PTC, the combination of dabrafenib (a BRAF inhibitor) and trametinib (a MEK inhibitor) has demonstrated clinical activity. Jeon et al. [26] reported an objective response rate of 73.1% with a median PFS of 21.7 months in patients with metastatic BRAF V600E-mutated PTC, although dose reduction was required in over 80% of patients. It should be noted that regulatory approval data for this combination are strongest in anaplastic thyroid carcinoma, and its use in BRAF-mutated DTC remains an area of evolving evidence [27]. The NCCN Version 1.2025 guidelines recommend somatic molecular testing for patients with advanced or progressive RR-DTC to identify actionable mutations and guide agent selection [6].
Importantly, not all patients with RR-DTC require immediate initiation of systemic therapy. For those with asymptomatic, slowly progressive disease, active surveillance with serial imaging at 3- to 6-month intervals may be appropriate, as the toxicity burden of kinase inhibitors can substantially impair quality of life. The decision to initiate systemic therapy is best guided by documented radiographic progression (by RECIST criteria), symptomatic disease, or disease threatening critical structures [2,4,6].
Guideline Recommendations
The 2015 ATA guidelines provide a comprehensive evidence-based framework for the management of DTC, including recurrence, and remain widely adopted in clinical practice [2]. The 2025 ATA guidelines represent a dedicated DTC-specific update that refines risk stratification, strengthens recommendations for molecular testing, and introduces response-adapted surveillance strategies while preserving the core management principles of the prior edition [4]. For cervical lymph node recurrences, the ATA recommends a risk-adapted approach: observation for small, stable, non-threatening nodes; confirmation by FNA cytology with or without FNA-Tg before intervention; and compartment-oriented surgery as the preferred therapeutic modality for resectable disease. RAI therapy is recommended for iodine-avid disease, and TSH suppressive therapy should be continued or intensified based on the response- to-therapy reclassification.
The NCCN Thyroid Carcinoma Version 1.2025 guidelines reinforce these principles and further emphasize the role of molecular testing in guiding systemic therapy for advanced and RR-DTC [6]. The NCCN recommends TSH suppression to below 0.1 mU/L for patients with persistent structural disease, periodic neck US and serum Tg monitoring, surgery for resectable recurrence, RAI for iodine-avid disease, and consideration of clinical trials or targeted systemic therapy for progressive RR-DTC. Collectively, these guidelines emphasize individualized decision-making within a multidisciplinary setting.
Conclusion
Recurrence of PTC, although not uncommon, is generally manageable when detected early and treated appropriately. Cervical lymph node metastasis represents the most frequent pattern of recurrence, and its diagnosis hinges on the combined use of neck US, serum Tg measurement, and FNA cytology with Tg washout analysis. Management encompasses a continuum of options, from active surveillance for indolent, small-volume nodal disease to compartment-oriented surgical reoperation, RAI therapy, external beam radiation, percutaneous ablation, and systemic targeted therapy for progressive RAI-refractory disease. The selection of the appropriate strategy demands careful consideration of disease biology, anatomic extent, molecular features, prior treatments, expected treatment morbidity, and patient preferences through shared decision-making. As molecular profiling becomes increasingly integrated into clinical practice and novel targeted agents continue to expand the therapeutic options, the outlook for patients with recurrent PTC may continue to improve. Adherence to evidence-based guidelines and multidisciplinary collaboration remain the cornerstones of optimal management.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
All work was done by JCL.