Evolution of recording methods in thyroid intraoperative neuromonitoring
Article information

Abstract
Intraoperative neuromonitoring (IONM) has been increasingly adopted as an adjunct to visual identification of the recurrent laryngeal nerve during thyroid surgery. The endotracheal tube (ETT)-based surface electrode system is the most widely established recording method; however, its dependence on stable electrode-vocal fold contact makes it vulnerable to false-positive loss-of-signal caused by tube displacement or rotation. These recording-side limitations have driven the development of alternative electrode configurations. Transcartilage electrodes, either needle or adhesive surface types, provide recordings independent of ETT position with less signal variation during tracheal displacement, but require surgical exposure of the thyroid cartilage. More recently, transcutaneous adhesive skin electrodes placed on the anterior neck have been introduced. Preclinical and early clinical studies have shown that these electrodes can record evoked laryngeal electromyography, with lower amplitudes than ETT electrodes but less waveform variation during tracheal displacement. A normative study identified sex, age, body mass index, and surgical extent as factors influencing amplitude, providing initial reference values for clinical use. However, whether conventional loss-of-signal criteria apply to these lower-amplitude recordings remains uncertain. This review focuses on the technical rationale, current evidence, and remaining barriers to clinical adoption of alternative recording methods for thyroid IONM.
Introduction
Thyroidectomy is widely performed for both malignant and benign thyroid disease. In patients with differentiated thyroid cancer, the most common thyroid malignancy, favorable long-term survival makes preservation of postoperative quality of life especially important [1]. The recurrent laryngeal nerve (RLN) innervates the intrinsic laryngeal muscles, principally the thyroarytenoid/vocalis muscle complex, and its injury during thyroidectomy produces clinically significant consequences [1,2]. Unilateral RLN palsy may cause dysphonia, ineffective cough, and increased aspiration risk; bilateral RLN palsy can compromise the airway and may require airway intervention, including tracheostomy in severe cases [2,3]. Reported rates of transient RLN palsy range from approximately 5% to 8%, and permanent palsy occurs in 0.3% to 3% of cases across systematic reviews and large clinical series [2-5].
Intraoperative neuromonitoring (IONM) was introduced to supplement visual nerve identification by providing real-time functional assessment of nerve integrity. The technique records evoked electromyography (EMG) from the laryngeal muscles during electrical stimulation of the RLN or vagus nerve (VN) and is used for nerve mapping, dissection guidance, and prognostication of postoperative vocal fold function [6]. As recording technology has evolved, several electrode configurations have been developed to reduce dependence on endotracheal tube (ETT) position, improve signal stability, or simplify intraoperative setup. This review traces the progression of IONM recording methods from conventional ETT-based electrodes through transcartilage approaches to transcutaneous adhesive skin electrodes, summarizes the available evidence for each, and identifies unresolved issues requiring further investigation. Figure 1 provides a schematic overview of the recording electrode configurations discussed in this review.
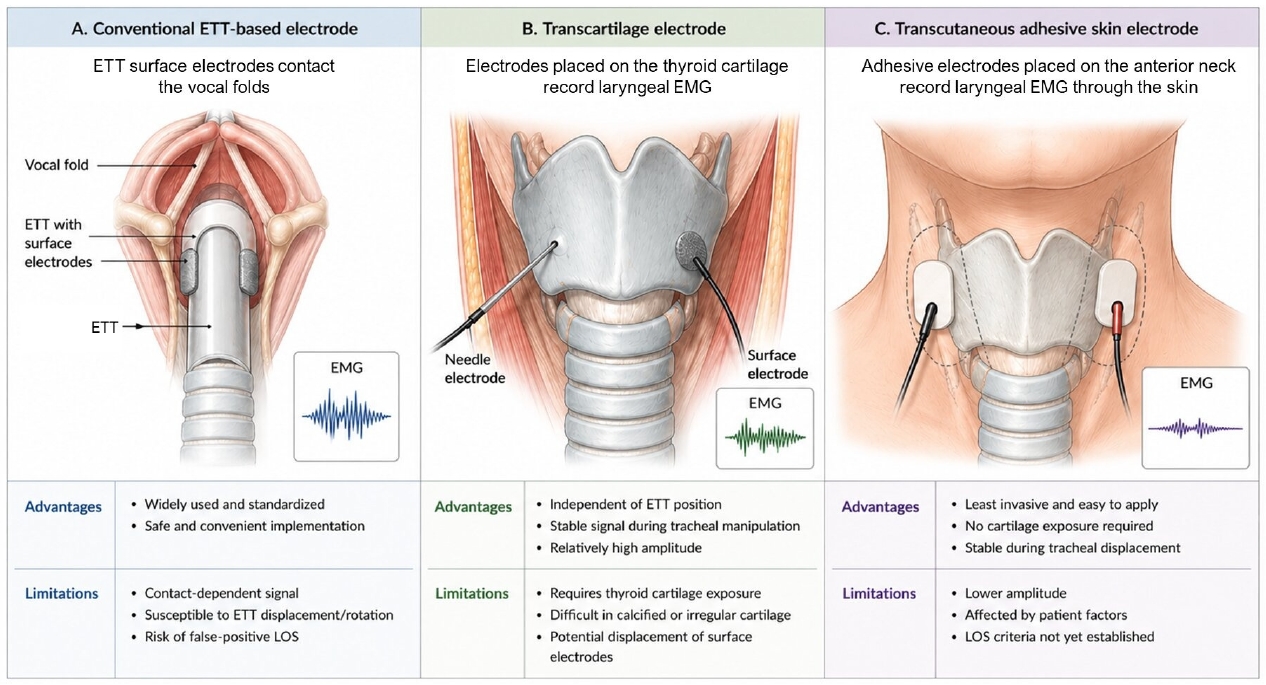
Recording electrode methods in thyroid intraoperative neuromonitoring. Schematic illustration of the three major recording electrode configurations discussed in this review. Conventional endotracheal tube (ETT)-based electrodes record laryngeal electromyography (EMG) through surface electrodes positioned at the level of the vocal folds. Transcartilage electrodes record EMG from electrodes placed on or through the thyroid cartilage, whereas transcutaneous adhesive skin electrodes record EMG through the anterior neck skin. Compared with ETT-based recording, transcartilage and transcutaneous approaches are less dependent on ETT position but have method-specific limitations, including the need for cartilage exposure, lower signal amplitude, electrode displacement, and unresolved loss-of-signal (LOS) criteria. Anatomical structures and waveforms are schematic and do not represent exact spatial or amplitude relationships.
Conventional Endotracheal Tube-Based Recording: Role and Limitations
The ETT-based surface electrode system is the most widely established method for recording laryngeal EMG during thyroid IONM. Paired stainless-steel surface electrodes embedded on the ETT are positioned so that they contact the vocal folds bilaterally, which enables standardized signal acquisition under appropriate electrode-vocal fold contact [6]. The 2011 international standards guideline by Randolph et al. [6] formalized the procedural framework for IONM, including equipment setup, stimulation parameters, the four-step monitoring sequence (V1, R1, R2, V2), and interpretation of loss-of-signal (LOS) events. Within this framework, the ETT-based surface electrode system has served as the conventional recording platform because of its safety, convenience, and applicability across institutions [6].
Despite wide use, ETT-based recording has well-recognized recording-side vulnerabilities. Signal quality depends on the degree of contact between the electrode surface and the vocal folds, and this contact is susceptible to disruption by tube rotation, vertical displacement, or interposition of secretions between the electrodes and the mucosa [7]. When electrode-vocal fold contact is lost, the result is a false-positive LOS: the monitor indicates an absent signal even though the nerve is functionally intact. Reported rates of IONM-related technical errors range from 3.8% to 23%, and ETT malposition is recognized as one of the leading causes [5,7]. A false-positive LOS can trigger unnecessary intraoperative management changes, including abandonment of the planned contralateral operation in a staged bilateral procedure. The troubleshooting algorithm described in the international standards guideline addresses this problem by requiring verification of equipment function, adequate stimulation current, and ETT position before a true neural LOS is accepted [6]. Nevertheless, verifying and repositioning the ETT intraoperatively require cooperation with the anesthesiologist and can be time-consuming, particularly in procedures where the trachea is mobilized or displaced [7].
Additional limitations include incompatibility with tracheostomy or non-standard airway conditions, in which ETT surface electrodes cannot be positioned against the vocal folds [8]. These recording-side limitations have provided the rationale for developing alternative electrode configurations that do not depend on ETT-vocal fold contact. The recording-side mechanism of false-positive LOS in ETT-based monitoring and the rationale for ETT-independent recording are summarized in Figure 2.
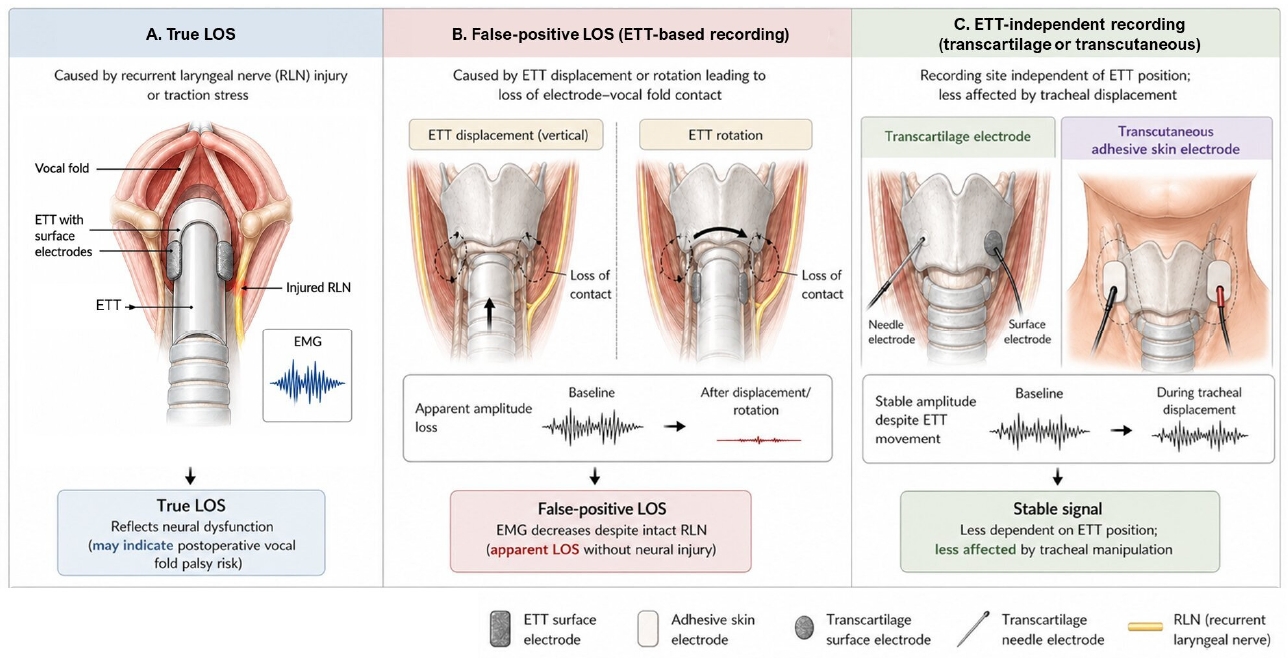
Mechanism of true and false-positive loss-of-signal (LOS) during thyroid intraoperative neuromonitoring. True LOS results from a genuine decrease in evoked laryngeal electromyography (EMG) associated with RLN injury or traction stress. False-positive LOS may occur in endotracheal tube (ETT)-based recording when ETT displacement or rotation disrupts electrode-vocal fold contact despite preserved RLN function. ETT-independent recording methods, including transcartilage and transcutaneous electrodes, are less affected by ETT position and tracheal displacement. Anatomical structures and waveforms are schematic and do not represent exact spatial relationships or amplitude ratios.
Transcartilage Recording Methods
1. Needle electrodes
Needle-based thyroid cartilage recording places electrodes in or near the subperichondrial region of the thyroid cartilage, providing a recording site closer to the laryngeal muscles and independent of ETT position [9-11]. Because the electrodes are fixed in the cartilage, their position does not change with tracheal movement or ETT displacement.
Chiang et al. [11] reported a clinical comparison of ETT electrodes and transcartilage needle electrodes in 110 patients (205 nerves at risk [NARs]). Both electrode types recorded evoked laryngeal EMG signals with comparable waveforms and latencies; however, the transcartilage needle electrodes showed significantly higher amplitudes and greater stability [11]. Importantly, both methods accurately detected partial and complete LOS events caused by traction stress, but only the ETT electrodes falsely detected LOS events caused by tube displacement during surgical manipulation [11]. This finding directly illustrates the advantage of recording that is independent of ETT position. Lee et al. [9] further demonstrated the feasibility of a single ipsilateral transcartilage needle electrode during unilateral hemithyroidectomy, confirming successful IONM in all NARs without LOS events and showing that adequate insertion depth is necessary for reliable signal acquisition.
The principal limitation of needle electrodes is that they require surgical exposure of the thyroid cartilage lamina and insertion under direct visualization. In patients with heavily calcified thyroid cartilage, common in older males, needle insertion may be difficult or unsuccessful.
2. Surface electrodes
An alternative transcartilage approach uses adhesive pre-gelled surface electrodes placed on the outer surface of the thyroid cartilage lamina. Wu et al. [12] evaluated this method in a porcine model and compared it with ETT electrodes. The transcartilage surface electrodes recorded typical evoked laryngeal EMG waveforms with amplitudes approximately 70% of ETT values. When upward tracheal displacement was experimentally induced, the transcartilage surface electrodes showed less variation in recorded EMG signals compared to ETT electrodes, while both electrode types accurately recorded progressive amplitude degradation during RLN traction stress. The authors noted that further electrode design optimization, particularly regarding shape, size, and adhesive stability, would be needed before clinical application [12].
Although transcartilage surface electrodes are technically simpler to apply than needle electrodes, they still require exposure of the thyroid cartilage surface and carry a risk of dislodgement during tissue manipulation. Clinical data on this approach remain limited.
Transcutaneous Adhesive Skin Electrodes
1. Preclinical evidence
Wu et al. [13] first evaluated transcutaneous adhesive skin electrodes for thyroid IONM in a porcine model. Evoked EMG was recorded simultaneously from ETT surface electrodes and from adhesive pre-gelled surface electrodes placed on the anterior neck skin overlying the larynx. The transcutaneous electrodes successfully recorded typical evoked laryngeal EMG waveforms, although amplitudes were substantially lower than those of ETT electrodes, approximately one-quarter to one-third of ETT values. The key finding was signal stability: when tracheal displacement was experimentally induced, the EMG signals obtained by ETT electrodes varied substantially, whereas those obtained by transcutaneous electrodes remained stable. Furthermore, when RLN traction stress was induced, both electrode types recorded the same pattern of progressively degrading amplitude with gradual recovery after release of traction, confirming that the transcutaneous approach accurately reflected nerve injury events. The authors concluded that transcutaneous recording was feasible but noted that new electrode designs would be needed to improve amplitudes before clinical application [13].
2. Clinical feasibility
Lee et al. [14] conducted the first clinical study of adhesive skin electrodes for RLN monitoring in 30 patients (39 NARs) undergoing thyroidectomy. Evoked EMG was recorded simultaneously from both a standard EMG tube and adhesive skin electrodes attached to the upper margins of the thyroid cartilage. IONM was successful in all NARs using the skin electrodes. Although amplitudes were significantly lower than those from the EMG tube, latencies were comparable between the two methods. A notable finding was that a small number of NARs showed false-positive LOS from the EMG tube during the monitoring steps, whereas all NARs monitored with adhesive skin electrodes maintained recordable biphasic EMG signals throughout. This observation supported the hypothesis that skin electrodes are less susceptible to contact-dependent signal loss. Electrode attachment required less than 1 minute and did not interfere with the surgical procedure [14].
3. Optimal attachment site
Shin et al. [15] investigated the optimal attachment location in both porcine models and human patients. Lateral attachment of adhesive skin electrodes on the thyroid cartilage lamina showed significantly higher evoked amplitudes than medial attachment in both preclinical and clinical settings [15]. The authors recommended attaching adhesive skin electrodes to the lateral side of the thyroid cartilage lamina, suggesting that placement closer to the cricoarytenoid joint may better capture activity of the intrinsic laryngeal muscles. In patients simultaneously monitored with both methods, skin electrode amplitudes were approximately one-third of EMG tube values, consistent with the preclinical observations [15].
4. Normative data and influencing factors
Shin et al. [16] subsequently reported the first normative EMG dataset for adhesive skin electrode-based IONM in a cohort of 167 patients (242 NARs). The study established that mean overall RLN and VN amplitudes recorded via skin electrodes correspond to approximately 32%-35% of reported ETT electrode amplitudes. No cases of LOS occurred during the study period, and all NARs yielded recordable biphasic waveforms [16].
The study’s principal contribution was the identification of clinical factors that significantly influence recorded amplitudes. In subgroup analyses, male sex, higher body mass index, age 55 years or older, and total thyroidectomy were associated with lower evoked amplitudes. The authors attributed these findings to greater distance between the skin electrode and the vocalis muscle in patients with thicker neck soft tissue, as well as to increased flap elevation range in total thyroidectomy, both of which increase signal attenuation through intervening tissue layers [16]. These subgroup differences suggest that skin electrode signals are particularly susceptible to attenuation by patient anatomy and surgical exposure, and that uniform amplitude thresholds may not be appropriate for all patients.
Remaining Limitations and Future Directions
Recent modifications of IONM recording methods have primarily aimed to reduce dependence on ETT position while simplifying electrode placement. Although transcartilage and transcutaneous approaches address several of the recording-side limitations of ETT-based IONM, their clinical adoption is still limited by unresolved issues in signal thresholding, electrode design, and outcome validation. In particular, transcutaneous adhesive skin electrodes should currently be regarded as an investigational or adjunctive recording method rather than a fully established stand-alone monitoring tool.
The conventional LOS threshold of 100 µV was established for ETT-based recordings, where baseline amplitudes typically exceed 500 µV [6,8]. Because adhesive skin electrodes produce amplitudes approximately one-third of ETT values, the 100 µV threshold may not be directly applicable. Lower baseline amplitudes may also complicate intraoperative decision-making, because a small absolute decrease in amplitude could be difficult to distinguish from signal attenuation or technical variability. This issue is particularly relevant when LOS influences decisions such as staged thyroidectomy or further nerve dissection. Establishing method-specific LOS criteria, and potentially patient-specific amplitude thresholds adjusted for sex, body mass index, and surgical extent, will be important before adhesive skin electrodes can be used as a stand-alone monitoring tool.
Because currently available adhesive electrodes were not specifically designed for thyroid cartilage recording, their size and shape may be suboptimal for placement over the anterior neck. Development of electrodes tailored for this anatomical region, with improved adhesion, contour conformity, and signal sensitivity, could increase recorded amplitudes and reduce variability.
The compatibility of transcutaneous recording with continuous IONM, which uses an implanted vagal electrode to provide repeated stimulation and dynamic EMG trend monitoring [17], has not been systematically evaluated. Whether the lower amplitudes achievable through the skin provide sufficient signal-to-noise ratio for reliable automated amplitude trending remains to be determined.
The existing clinical evidence is derived from single-center studies with relatively limited sample sizes. Multicenter comparative studies evaluating diagnostic accuracy, including sensitivity and specificity for predicting postoperative vocal fold palsy, are needed. Future studies should also compare postoperative RLN palsy rates in patients monitored with ETT versus alternative electrodes to determine whether position-independent recording translates into measurable clinical benefit.
Conclusion
The main technical limitation of conventional IONM recording is its dependence on stable ETT-vocal fold contact, and recent alternative electrodes have largely been developed to overcome this recording-side vulnerability. Transcartilage electrodes, both needle and surface types, were less affected by tracheal or tube displacement than ETT electrodes in experimental or clinical comparisons but require surgical exposure of the thyroid cartilage and may be limited by cartilage calcification or electrode dislodgement. Transcutaneous adhesive skin electrodes represent the least invasive alternative, allowing rapid setup and stable recording. Early clinical studies demonstrated their feasibility, identified the lateral thyroid cartilage lamina as the preferred attachment site, and provided the first normative dataset demonstrating that patient-related and surgical factors significantly influence recorded amplitudes. They may also reduce device-related costs compared with EMG tubes, although formal cost-effectiveness analyses remain limited. Therefore, despite the limitations of contact-dependent recording, ETT-based surface electrodes remain the current standard method for thyroid IONM. Before these alternative recording methods can be incorporated into standardized IONM protocols or used as stand-alone approaches, method-specific LOS thresholds, optimized electrode designs, and prospective outcome data are needed.
Notes
Funding
None.
Conflict of Interest
Eui-Suk Sung is the Associate Editor of the journal, but was not involved in the review process of this manuscript. Otherwise, there is no conflict of interest to declare.
Data Availability
None.
Author Contributions
All work was done by ESS.