Needle tract seeding of thyroid cancer: incidence, risk factors, and technical considerations
Article information

Abstract
Fine-needle aspiration cytology (FNAC) is widely used for the diagnostic evaluation of thyroid nodules and has a well-established safety profile. Needle tract seeding (NTS) is an exceptionally rare complication reported mainly in retrospective institutional series and case reports. Reported incidence ranges from 0.02% to 0.19% across large retrospective cohorts. Papillary thyroid carcinoma accounts for most reported cases, whereas follicular and anaplastic thyroid carcinomas may be relatively overrepresented on a per-case basis, although this observation is limited by small case numbers. The latency between initial aspiration and clinical detection of NTS ranges from several months to over a decade. NTS typically presents as a superficial neck nodule along a previous needle trajectory, and histopathologic confirmation is generally required to distinguish it from benign subcutaneous lesions. Surgical excision has achieved favorable local control in most reported cases, while overall prognosis appears to reflect the biological behavior of the primary tumor. Technical measures such as small-gauge needles, limited passes, non-aspiration or hybrid sampling, and careful withdrawal may reduce theoretical risk, but direct preventive evidence remains lacking. FNAC remains a safe and essential diagnostic procedure despite this rare complication.
Introduction
Fine-needle aspiration cytology (FNAC) is widely used as a first-line diagnostic procedure for thyroid nodules and is recommended by multiple international and domestic guidelines, including the American Thyroid Association management guidelines and the Korean Society of Thyroid Radiology (KSThR) consensus statement on ultrasound-guided fine-needle aspiration [1-3]. The procedure is generally regarded as safe, with most complications limited to local pain, minor hematoma, and transient vasovagal reactions.
Needle tract seeding (NTS), also referred to as needle tract implantation (NTI), denotes the deposition and subsequent growth of viable tumor cells along the path traversed by the biopsy needle. Although this phenomenon has been well recognized in other malignancies such as hepatocellular carcinoma, pancreatic cancer, breast cancer, and lung cancer, its occurrence following thyroid FNAC has been considered exceedingly uncommon. Nevertheless, a growing number of case reports and several institutional series have documented NTS following aspiration of both primary thyroid cancers and metastatic cervical lymph nodes.
The purpose of this article is to present a narrative review of the available literature on NTS after thyroid FNAC, including its reported incidence, histological distribution, clinical features, outcomes, and procedural risk factors.
Epidemiology
Three principal studies have provided incidence estimates for NTS following thyroid FNAC. Cappelli et al. [4] retrospectively reviewed 7,449 consecutive thyroid fine-needle aspirations (FNAs) and identified a single case of tumor seeding, yielding an incidence of approximately 0.02%. Ito et al. [5] reported seven cases of NTI among 4,912 patients with papillary thyroid carcinoma (PTC) who had undergone preoperative FNA, corresponding to an incidence of 0.14%. The largest series to date is that of Hayashi et al. [6], who identified 22 cases of NTI among 11,745 thyroid cancer patients (0.19%) and an additional eight cases among 2,193 patients who underwent aspiration of metastatic cervical lymph nodes (0.36%). The reported incidence estimates from these studies are summarized in Table 1.
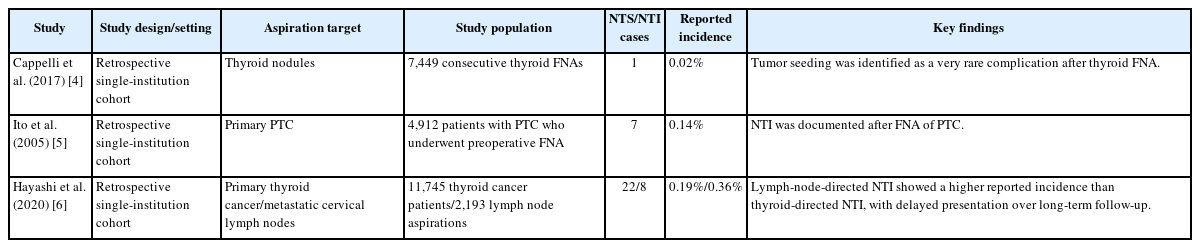
Reported incidence of NTS or implantation after thyroid FNA
The cumulative incidence appears to increase with duration of follow-up, indicating that NTS may be detected only after prolonged surveillance. In the Hayashi et al. [6] series, the cumulative incidence of thyroid-directed NTI increased from 0.15% at 5 years to 0.37% at 10 years, while lymph-node-directed NTI increased from 0.37% to 0.58% over the same interval. These figures suggest that a proportion of NTS lesions develop subclinically and become apparent only with extended observation.
It should be noted that all available incidence data derive from retrospective single-institution series, and the true incidence may differ depending on procedural technique, follow-up duration, and case ascertainment methods.
Histological Distribution
Among reported cases, PTC accounts for the majority of NTS events. In the Hayashi et al. [6] series, PTC was responsible for 16 of 22 thyroid-directed NTI cases; however, when expressed as a proportion of aspirated tumors of each subtype, the incidence was notably higher for follicular thyroid carcinoma (FTC) and anaplastic thyroid carcinoma (ATC). The subtype-specific incidence was 0.1% for PTC, 1.2% for FTC, and 1.7% for ATC.
These findings suggest that NTS may be relatively overrepresented in follicular and anaplastic carcinomas on a per-case basis, although this observation should be interpreted cautiously because of the small number of reported cases. Individual case reports have further documented NTS of FTC presenting years after the initial aspiration [7]. However, the absolute numbers of FTC and ATC cases in this series were small, and the confidence intervals surrounding these estimates are correspondingly wide. In the Hayashi et al. [6] series, no cases of NTS were identified following aspiration of poorly differentiated thyroid carcinoma or medullary thyroid carcinoma, although the reason for this finding remains uncertain.
Clinical Presentation
NTS typically presents as one or more subcutaneous nodules located along the trajectory of the previous biopsy needle. Reported lesions have been found in the dermis, subcutaneous fat, and strap musculature, with the subcut
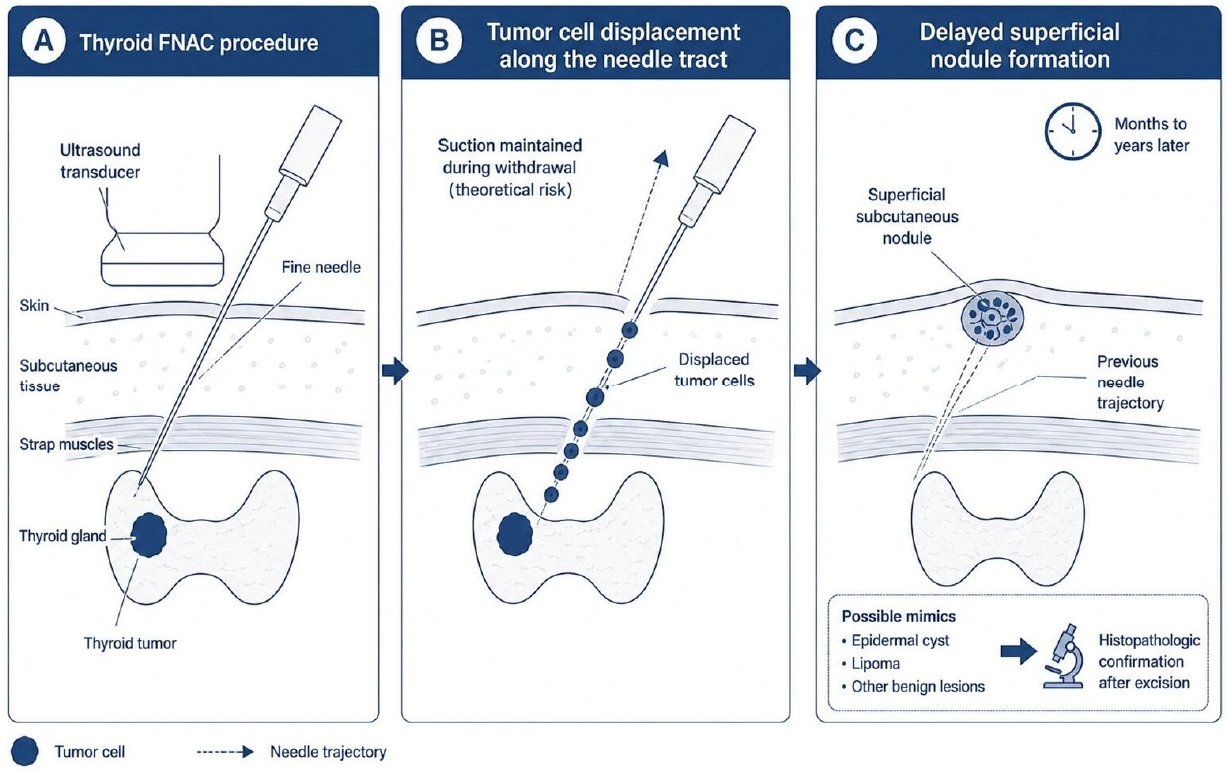
Figure 1. Schematic representation of NTS after thyroid FNAC. During aspiration of a thyroid malignancy, viable tumor cells may be displaced along the needle trajectory, particularly when negative pressure is maintained during needle withdrawal. These cells may remain within the dermis, subcutaneous tissue, or strap musculature and later develop into superficial nodules near the previous puncture site. Because these lesions may mimic benign entities such as epidermal cysts or lipomas, histopathologic confirmation after excision is often required. FNAC, fine-needle aspiration cytology; NTS, needle tract seeding.
Schematic representation of NTS after thyroid FNAC. During aspiration of a thyroid malignancy, viable tumor cells may be displaced along the needle trajectory, particularly when negative pressure is maintained during needle withdrawal. These cells may remain within the dermis, subcutaneous tissue, or strap musculature and later develop into superficial nodules near the previous puncture site. Because these lesions may mimic benign entities such as epidermal cysts or lipomas, histopathologic confirmation after excision is often required. FNAC, fine-needle aspiration cytology; NTS, needle tract seeding.
aneous layer being the most common site. In some cases, multiple discrete lesions are present along a single needle tract. Clinically, these nodules may be mistaken for epidermal cysts or lipomas, particularly when the interval from the original biopsy is long [8]. A schematic overview of tumor cell displacement along the needle trajectory and delayed superficial nodule formation is shown in Figure 1.
The latency between the index aspiration and clinical detection of NTS is highly variable. Reported intervals in the Hayashi et al. [6] series ranged from under 1 year to nearly a decade for thyroid-directed cases, with a shorter median interval for lymph-node-directed cases [6]. An extreme example was reported by Ando et al. [9], in which NTS of PTC was diagnosed 18 years after the initial surgery, highlighting the potential for very prolonged subclinical growth.
Diagnosis is typically confirmed by histopathological examination of the excised nodule, with immunohistochemical positivity for thyroglobulin and TTF-1 supporting thyroid origin. Cytological evaluation of the subcutaneous nodule by repeat FNA may also suggest the diagnosis, although tissue confirmation is generally preferred.
For practicing physicians, a newly detected superficial neck nodule located near a previous needle trajectory should prompt consideration of NTS, particularly in patients with a history of thyroid malignancy or lymph node aspiration. In such cases, careful review of the prior FNAC route, targeted ultrasonographic assessment, and histopathological confirmation after excision or biopsy may help distinguish NTS from benign lesions such as epidermal cysts or lipomas.
Outcomes
In most reported cases, surgical excision has been performed and has achieved favorable local control. In the Hayashi et al. [6] series, all identified patients with thyroid-directed NTI underwent salvage excision, and no local recurrence of the seeded lesion itself was documented. However, a substantial proportion of these patients subsequently developed distant metastases or died of disease, reflecting the aggressive biology of the underlying primary cancer rather than failure of local treatment for NTS.
Outcomes in lymph-node-directed NTI appeared more favorable overall, with a higher proportion of patients remaining disease-free after excision [6]. This difference likely reflects the generally less aggressive tumor biology in patients whose disease is confined to cervical lymph nodes at the time of aspiration.
These observations suggest that while NTS itself is amenable to surgical treatment, its prognostic significance is largely determined by the stage and biology of the primary malignancy.
Risk Factors
Risk factors for NTS may be broadly categorized as tumor-related and procedure-related.
1. Tumor-related factors
Aggressive histological subtypes (FTC, ATC), larger tumor size, loss of cellular cohesion, and high proliferative activity have been proposed as features that may predispose to implantation along the needle tract. The observation that the proportional incidence of NTS appears higher in FTC and ATC is consistent with this hypothesis, although the small sample sizes preclude definitive conclusions.
2. Procedure-related factors
The systematic review by Polyzos and Anastasilakis [10] proposed a practical hierarchy of procedural measures that may influence the risk of NTS. According to this framework, the use of small-gauge needles (25 G for solid nodules, 23 G for cystic components) and a limited number of passes are considered preferred practice. The use of a non-aspiration (capillary) technique or the release of suction before needle withdrawal is regarded as acceptable and theoretically protective, although direct evidence that these measures reduce NTS is lacking.
Conversely, the use of large-bore needles, an excessive number of passes (generally considered as more than five), and maintaining negative pressure during needle withdrawal are discouraged, as these maneuvers may theoretically increase the volume of displaced tumor cells. Proposed tumor-related and procedure-related factors, together with technical considerations for reducing the theoretical risk of NTS, are summarized in Table 2.
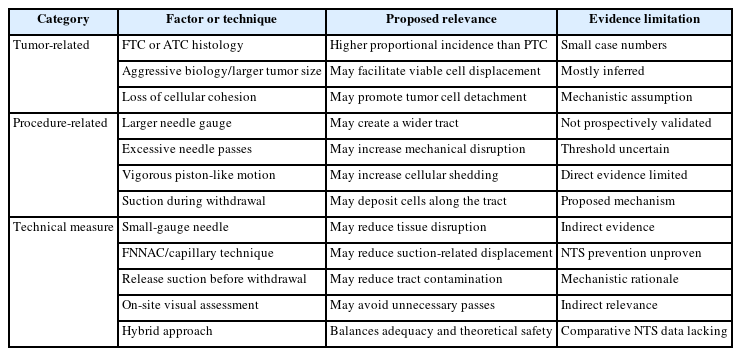
Proposed risk factors and technical considerations for reducing the theoretical risk of NTS
Technical Considerations
Several procedural modifications have been proposed to decrease the amount of cellular material deposited along the needle tract and thereby reduce the theoretical possibility of implantation, although their preventive effect against NTS has not been directly demonstrated. The use of fine-needle non-aspiration cytology (FNNAC), in which specimen collection relies on capillary action rather than applied suction, may reduce the theoretical risk of NTS by limiting the volume of aspirated material and by avoiding sustained negative pressure during needle withdrawal. Meta-analytic data suggest that the diagnostic performance of FNNAC is comparable to that of conventional FNAC for thyroid nodules [11], making it a viable alternative in clinical practice. A prospective randomized trial similarly demonstrated that both techniques provide adequate diagnostic yield, although FNAC may produce a higher rate of determinate results [12]. However, direct evidence demonstrating a reduced rate of NTS with FNNAC is currently lacking; indeed, at least one case of NTS has been reported even after fine-needle capillary biopsy without aspiration [13].
Notably, these comparative studies were conducted using conventional smear techniques, whereas liquid-based cytology (LBC) is now widely adopted in clinical practice. In conventional smears, a portion of the sampled material may remain within the needle hub after slide preparation. In contrast, LBC involves rinsing the needle, allowing more complete recovery of cellular material into the specimen. In addition, LBC is less affected by blood contamination, which may facilitate cytological interpretation even in bloody samples. In this context, the conventional recommendation to release suction prior to needle withdrawal to reduce the risk of NTS may warrant reconsideration, as maintaining negative pressure throughout the procedure, including during withdrawal, may improve cellular yield in the LBC era, although its impact on NTS risk remains uncertain. In practice, however, maintaining constant negative pressure requires sustained effort, and suction may be inadvertently released during needle withdrawal, raising concerns about potential NTS. Furthermore, although LBC is relatively less affected by blood contamination, excessive specimen volume may still compromise diagnostic adequacy, particularly when it exceeds approximately 1 mL [14]. In hypervascular nodules, aspiration often yields large volumes of blood, which may adversely affect specimen quality. In this setting, achieving an optimal balance between adequate cellularity and minimal blood contamination becomes critical. On-site visual assessment of specimen adequacy may facilitate this balance. As described by Yoo et al. [14], evaluation of specimen color, volume, and particle count can guide the operator in determining the need for additional passes. Consistent with this concept, the KSThR consensus statement recommends a hybrid approach, in which initial capillary sampling is followed by aspiration when specimen adequacy is insufficient on visual assessment.
It should be emphasized that no prospective comparative study has directly evaluated the effect of any single procedural modification on the incidence of NTS, specimen adequacy, and diagnostic accuracy in the LBC era, and current recommendations are based primarily on theoretical considerations and expert consensus.
Conclusion
NTS following thyroid FNAC is a rare complication with a reported incidence of 0.02% to 0.19% in available retrospective series. PTC accounts for most cases, while FTC and ATC may be relatively overrepresented on a per-case basis, although this observation is limited by small case numbers. Latency may extend from several months to nearly two decades. Surgical excision has achieved favorable local control in most reported cases, while overall prognosis is primarily determined by the biology of the underlying malignancy. Procedural modifications, including the use of small-gauge needles, a limited number of passes, non-aspiration or hybrid sampling techniques, and release of suction before needle withdrawal, represent reasonable measures that may mitigate the theoretical risk of NTS, though direct supporting evidence remains absent. Until such evidence becomes available, NTS should be considered during long-term surveillance when a superficial neck nodule develops along a previous needle trajectory, particularly in patients with aggressive tumor histology or extensive lymph node metastases. During preprocedural counseling, patients may be informed that FNAC remains a safe and essential diagnostic procedure, and that NTS is an exceptionally rare complication. Prospective studies are needed to define the optimal balance between cellular adequacy and procedural safety in the LBC era.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
All work was done by SYA.