Thyroid nodule ultrasonography: promising commercial AI tools and challenges in specificity and generalizability
Article information

Abstract
Thyroid nodules are common findings in clinical practice, detectable in 19%-68% of the general population by high-resolution ultrasonography (US). Accurate risk stratification is essential to identify the 7%-15% of nodules harboring malignancy while avoiding unnecessary fine-needle aspiration biopsies. Standardized reporting systems such as the American College of Radiology Thyroid Imaging Reporting and Data System and the Korean Thyroid Imaging Reporting and Data System were developed to improve consistency and reduce unnecessary biopsies, yet interobserver variability persists. Artificial intelligence (AI), particularly convolutional neural network-based deep learning, has been increasingly evaluated as a tool for automated image analysis, feature extraction, and risk assessment of thyroid nodules on US. As of early 2026, six AI platforms for assessing thyroid nodule sonograms have received U.S. Food and Drug Administration clearance. Published studies suggest that many of these systems can achieve sensitivity comparable to that of experienced radiologists, with potential incremental value for less experienced operators. This review examines the current landscape of commercially available AI tools for thyroid US, compares their diagnostic performance, discusses limitations, and identifies priorities for future research, with emphasis on external validation and alignment with regional risk stratification systems.
Introduction
Thyroid nodules are frequently encountered in routine clinical practice. Population-based studies using high-resolution ultrasonography (US) have shown that thyroid nodules can be detected in 19%-68% of randomly selected individuals, with higher prevalence among women and the elderly [1]. In South Korea, thyroid cancer has been the most frequently diagnosed cancer since 2019 and was ranked first overall in 2021 with 35,303 new cases, partly associated with the widespread adoption of screening US [2]. The clinical significance of thyroid nodules lies in the need to exclude thyroid cancer, which occurs in approximately 7%-15% of all nodules depending on age, sex, radiation exposure history, and family history [1].
To standardize the assessment of thyroid nodules and guide biopsy decisions, several risk stratification systems (RSS) have been developed. The American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS), published in 2017, uses a point-based system to assign nodules to one of five risk categories based on composition, echogenicity, shape, margin, and echogenic foci [3]. In Korea, the Korean Society of Thyroid Radiology developed the Korean Thyroid Imaging Reporting and Data System (K-TIRADS), most recently revised in 2021, which uses a pattern-based approach to risk stratification [4]. These systems were designed to reduce unnecessary biopsies and improve reporting consistency, yet interobserver variability in the assessment of US features remains well documented, and the accuracy of nodule characterization continues to be operator-dependent [3,5].
In this context, artificial intelligence (AI), particularly deep learning methods based on convolutional neural networks (CNNs), has been applied to thyroid nodule US with the goal of improving diagnostic consistency and reducing operator dependence. As of early 2026, six AI platforms for assessing thyroid nodule sonograms have received U.S. Food and Drug Administration (FDA) clearance [6]. This review examines the current landscape of these commercially available tools, summarizes the published evidence on their diagnostic performance, and discusses the challenges and future prospects of AI in thyroid US diagnosis.
Overview of Artificial Intelligence in Medical Imaging
Modern AI-based image analysis relies predominantly on deep learning, a subset of machine learning (ML) that uses multilayered neural networks to learn hierarchical representations directly from raw pixel data. Among deep learning architectures, the CNN has been the most widely adopted for image classification tasks, including the evaluation of thyroid nodules [7]. In a typical CNN-based workflow for thyroid US, the network is trained on thousands of annotated US images, each labeled with pathology-confirmed diagnoses. Once trained, the network can classify new images within seconds, reducing reliance on predefined handcrafted imaging features [7,8].
The number of FDA-authorized AI/ML-enabled medical devices has grown rapidly in recent years, with the majority in the field of radiology [9]. The FDA maintains a continuously updated list of these devices, though the agency notes that the list may not be comprehensive [10]. In Korea, the number of AI-based medical software products has similarly increased, and efforts are underway to develop AI tools that integrate directly with the K-TIRADS framework, an important consideration given that most globally available products are trained on ACR TI-RADS or other non-Korean classification systems [11]. The general workflow of AI-assisted thyroid nodule assessment on US is summarized in Figure 1.
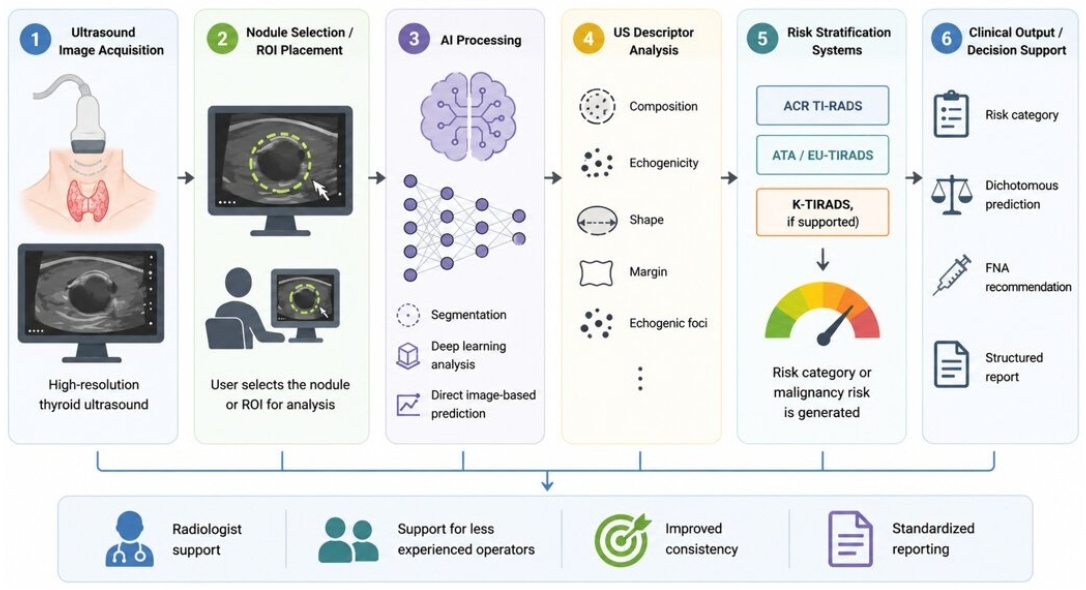
General workflow of AI-assisted thyroid nodule assessment on ultrasonography. AI-assisted thyroid US evaluation typically begins with high-resolution image acquisition and user-defined nodule or ROI selection. Depending on the system, AI processing may include segmentation, deep learning-based image analysis, descriptor assignment, or direct image-based prediction. The resulting outputs may be mapped to risk stratification systems such as ACR TI-RADS, ATA/EU-TIRADS, or K-TIRADS when supported. These outputs can support clinical decision-making by providing risk categories, dichotomous predictions, FNA recommendations, and structured reports. AI, artificial intelligence; ROI, region of interest; ACR TI-RADS, American College of Radiology Thyroid Imaging Reporting and Data System; ATA, American Thyroid Association; EU-TIRADS, European Thyroid Imaging Reporting and Data System; K-TIRADS, Korean Thyroid Imaging Reporting and Data System; FNA, fine-needle aspiration; US, ultrasound.
Commercially Available Artificial Intelligence Tools for Thyroid Nodule Interpretation
A 2026 review by Thomas and Tessler [6] identified six FDA-cleared AI platforms for assessing thyroid nodule sonograms as of early 2026. Among the most widely discussed in the literature are S-Detect (Samsung Medison), AmCAD-UT (AmCAD BioMed), Koios DS (Koios Medical), Medo-Thyroid (Medo AI), See-Mode SMART-T (See-Mode Technologies), and PIUR tUS Infinity (PIUR Imaging). Each product differs in its platform, workflow integration, classification approach, and intended clinical role. Some systems, such as S-Detect, AmCAD-UT, and Koios DS, primarily support risk stratification or diagnostic decision-making, whereas others, such as Medo-Thyroid, See-Mode SMART-T, and PIUR tUS Infinity, are more focused on segmentation, measurement, documentation, or structured reporting support. The evidence base varies considerably across products. S-Detect and AmCAD-UT have accumulated the most independent clinical studies, and Koios DS has FDA submission-based performance data supplemented by limited external evidence. Medo-Thyroid, See-Mode SMART-T, and PIUR tUS Infinity have more limited published validation data at this time. Table 1 summarizes the main characteristics of FDA-cleared AI platforms for thyroid nodule sonography.
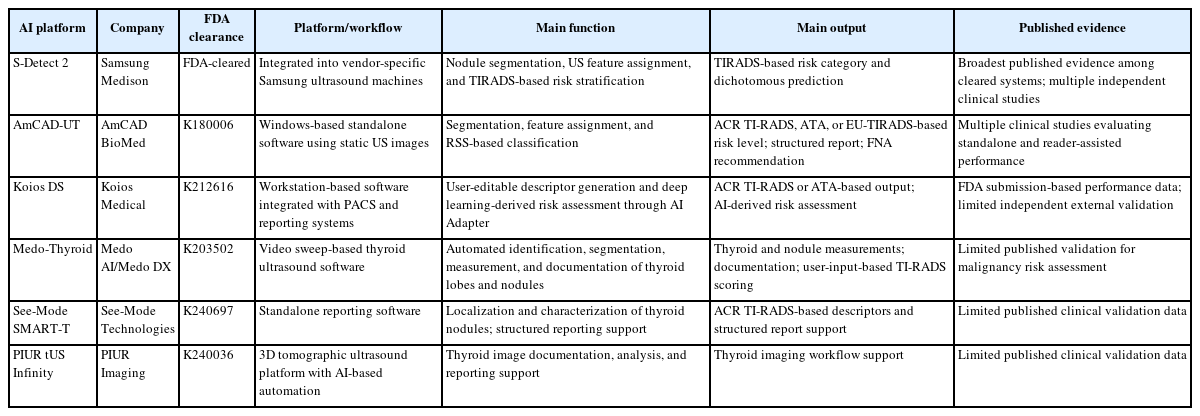
FDA-cleared AI platforms for thyroid nodule sonography as of early 2026
S-Detect
S-Detect 2 (Samsung Medison) is a deep learning-based system integrated directly into vendor-specific Samsung US machines. During scanning, the operator freezes the image and manually draws a region of interest (ROI) around a nodule. The system then performs automated segmentation and assigns six US features (composition, orientation, echogenicity, shape, borders, and calcifications) from which it generates a TIRADS-based risk stratification and a dichotomous prediction (probably benign vs. probably malignant) [8].
S-Detect has accumulated the broadest evidence base among cleared systems, with more than 12 independent evaluations published to date [8,12-17]. A recurring finding across these studies is that while sensitivity is high, specificity tends to be lower than that of experienced radiologists. In the largest study, Han et al. [12] analyzed 454 nodules and compared S-Detect to a single experienced radiologist using K-TIRADS classification. S-Detect achieved a sensitivity of 97.6% (matching the radiologist), but its specificity (21.6%) and accuracy (49.6%) were significantly lower (radiologist: 36.2% and 58.8%, respectively). The dichotomous prediction produced more balanced results: 81.4% sensitivity and 81.9% specificity [12]. This pattern suggests that TIRADS-based feature assignment by AI may overcall suspicious features, whereas the end-to-end dichotomous prediction better balances sensitivity and specificity for clinical decision-making.
Kim et al. [13] evaluated S-Detect in a study of 218 nodules and reported sensitivity of 81.4%, specificity of 68.2%, and overall accuracy of 73.4% for the dichotomous prediction. When the radiologist used S-Detect as an aid, sensitivity increased from 84.9% to 93.0%, but specificity decreased from 96.2% to 67.4% [13]. This trade-off is clinically relevant because AI assistance may reduce missed malignancies but may also increase unnecessary fine-needle aspiration (FNA) or follow-up if the AI output is accepted uncritically.
To address whether AI benefits operators at different experience levels, Chung et al. [14] compared S-Detect to a radiology resident, fellow, and attending radiologist in a sample of 165 nodules. The CAD system showed accuracy (88.5%) similar to that of the resident and fellow (83.0% each) but lower than the attending (95.8%). All three readers showed slight, non-significant improvements when assisted by S-Detect [14]. These findings suggest that the main clinical value of AI assistance may be standardization of interpretation for less experienced operators rather than replacement of expert thyroid radiologists.
AmCAD-UT
AmCAD-UT (AmCAD BioMed) is a Windows-based standalone software that analyzes static US images after image acquisition. It received FDA 510(k) clearance (K180006) as a computer-aided detection device for thyroid nodules [18]. The user defines an approximate nodule boundary, after which automated segmentation generates feature assignments (echogenicity, echogenic foci, texture, margin, and shape) and a risk level according to user-selectable RSS including ACR TI-RADS, American Thyroid Association (ATA), and European Thyroid Imaging Reporting and Data System (EU-TIRADS). A structured report and FNA recommendation are automatically generated, and the software allows adjustment of detection sensitivity settings for individual features [8].
Reverter et al. [15] evaluated AmCAD-UT using 300 nodules and compared the system to a thyroid US expert. The AI tool matched the expert in sensitivity (87.0%) but had lower specificity (68.8% vs. 91.2%) and a lower area under the receiver operating characteristic curve (AUC: 0.72 vs. 0.88). The difference in negative predictive value was not significant (86.3% vs. 90.9%) [15].
Lu et al. [16] used AmCAD-UT to analyze 234 intermediate-risk nodules (TIRADS categories 3 and 4) and compared performance among the AI system, radiologists, and AI-assisted radiologist reads. They reported an AUC of 0.916 for AmCAD-UT compared with 0.653 for radiologists alone, with an increase to 0.93 when radiologists used the software [16]. Wu et al. [17] conducted a multi-reader multi-case study with 19 physicians and 265 nodules and found that the mean AUC increased from 0.728 without AI to 0.792 with AI assistance, with a concomitant reduction in inter-observer variability. These results indicate that AmCAD-UT’s principal strength may lie in reducing reader-to-reader variation and supporting less experienced sonographers rather than outperforming experienced specialists.
Koios DS
Koios DS (Koios Medical) is a workstation-based software that integrates with picture archiving and communication system (PACS) and reporting systems. It received FDA 510(k) clearance (K212616) in December 2021 for both breast and thyroid ultrasound functionality [19]. Users select two orthogonal ROIs representing a single nodule, after which the software generates user-editable nodule descriptors (composition, echogenicity, shape, margin, and echogenic foci) mapped to ACR TI-RADS or ATA criteria. An advanced feature called "AI Adapter" provides a deep learning-derived risk assessment independent of the descriptor-based output, which can upgrade or downgrade the initial RSS categorization [19].
According to its FDA submission, the thyroid engine was validated on 500 nodules. When applied with ACR TI-RADS guidelines, the AI Adapter and descriptor predictors achieved an AUC of 79.8%, showing improved performance compared with the average physician AUC in the FDA submission. In a separate multi-reader multi-case clinical trial with 15 readers and 650 nodules, the system demonstrated a mean AUC improvement of 0.083 (95% confidence interval, 0.066-0.099) when readers used Koios DS compared with unassisted reads [19]. Independent external validation studies remain limited compared with S-Detect and AmCAD-UT.
Medo-Thyroid
Medo-Thyroid (Medo DX) received FDA 510(k) clearance (K203502) in April 2021. According to its FDA summary, the device is designed to view and quantify ultrasound thyroid image data using ML techniques to aid in analysis, quantification, and documentation of thyroid lobes and nodules. The user obtains video sweeps of each side of the thyroid gland, and the software uses AI to automatically identify the thyroid and any nodules, generate measurements, and create documentation. TI-RADS scoring remains based on the user’s manual input rather than automated malignancy prediction [20]. In its current form, Medo-Thyroid functions primarily as an automated segmentation and measurement tool and is not equivalent to fully automated risk assessment systems.
See-Mode SMART-T and PIUR tUS Infinity
See-Mode Augmented Reporting Tool, Thyroid (SMART-T) received FDA 510(k) clearance (K240697) in 2024 [21]. According to its FDA summary, SMART-T is a standalone reporting software that assists with localization and characterization of thyroid nodules, provides ACR TI-RADS-based descriptors, and supports structured reporting. PIUR tUS Infinity (PIUR Imaging) received FDA 510(k) clearance (K240036) and combines three dimensional tomographic ultrasound technology with AI-based automation for thyroid image documentation, analysis, and reporting [22]. Published clinical validation data for both systems are still limited at the time of writing, though both represent the expanding landscape of cleared AI tools for thyroid US. Table 2 summarizes representative clinical studies evaluating the diagnostic performance of AI tools for thyroid nodule ultrasound.
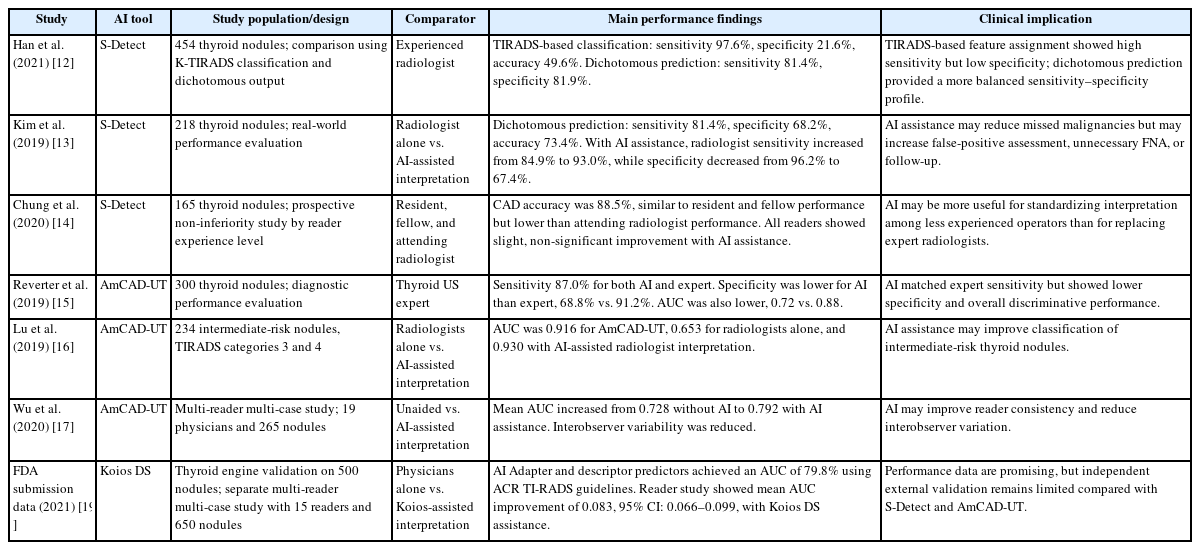
Representative studies evaluating diagnostic performance of AI tools for thyroid nodule ultrasound
Comparison of Diagnostic Performance
Across available studies, a recurring pattern is that most AI tools achieve sensitivity comparable to that of experienced radiologists for thyroid cancer detection, although this depends on the threshold, dataset, and reader comparator used in each study. Specificity remains a challenge for most systems, with experienced radiologists generally outperforming algorithms in standalone comparisons. This is clinically relevant because lower specificity may increase false-positive assessments, leading to unnecessary FNA, additional follow-up examinations, patient anxiety, and increased clinical workload [8,12,15]. The greatest performance gains from AI appear to accrue to less experienced operators, a finding consistent across studies using both S-Detect and AmCAD-UT [14,16,17]. This suggests a possible clinical deployment model in which AI tools serve as an adjunctive support tool for less experienced operators in settings without dedicated thyroid imaging expertise, while adding less incremental value in highly specialized centers where senior radiologists already achieve high accuracy.
An additional observation is that dichotomous predictions (benign vs. malignant) tend to produce more balanced sensitivity-specificity trade-offs than TIRADS-based feature assignments [8,12]. One explanation is that feature-by-feature TIRADS assignment amplifies overcalling of suspicious descriptors, whereas end-to-end deep learning predictions integrate all image information simultaneously and may better reflect overall malignancy risk.
Limitations of Current Artificial Intelligence Tools
Despite accumulating evidence, current AI tools for thyroid US have several notable limitations. First, commercially available thyroid nodule tools are generally not designed to detect non-nodular thyroid pathology (e.g., diffuse thyroiditis) or assess cervical lymph nodes, limiting their utility in comprehensive thyroid evaluations [6,8]. Second, the reliability of AI output depends substantially on image quality and acquisition technique, meaning that suboptimal images will yield unreliable classifications regardless of the underlying algorithm [8].
Third, and of particular relevance to Korean clinical practice, most available systems were trained on and designed around Western classification systems (ACR TI-RADS, ATA, EU-TIRADS). K-TIRADS, which is the standard system used in Korea, employs a different pattern-based classification approach [4]. As Kwak [11] has noted, the absence of K-TIRADS integration in currently available cleared products represents a meaningful gap for Korean practitioners.
Fourth, most cleared AI products have limited interpretability. Although feature-based outputs (e.g., TIRADS descriptors) provide some degree of transparency, the deep learning engines underlying systems such as the dichotomous prediction of S-Detect and the AI Adapter of Koios DS do not provide transparent decision pathways for clinicians [8]. This lack of interpretability may affect clinician trust and complicate medicolegal considerations.
Finally, ongoing post-market surveillance is important. While FDA clearance provides an initial assurance of safety and efficacy, AI performance can degrade when applied to populations or imaging equipment different from those used in training data [23]. Practices adopting these tools should monitor performance metrics over time. The key clinical implications, limitations, and future directions of AI-assisted thyroid US are summarized in Figure 2.
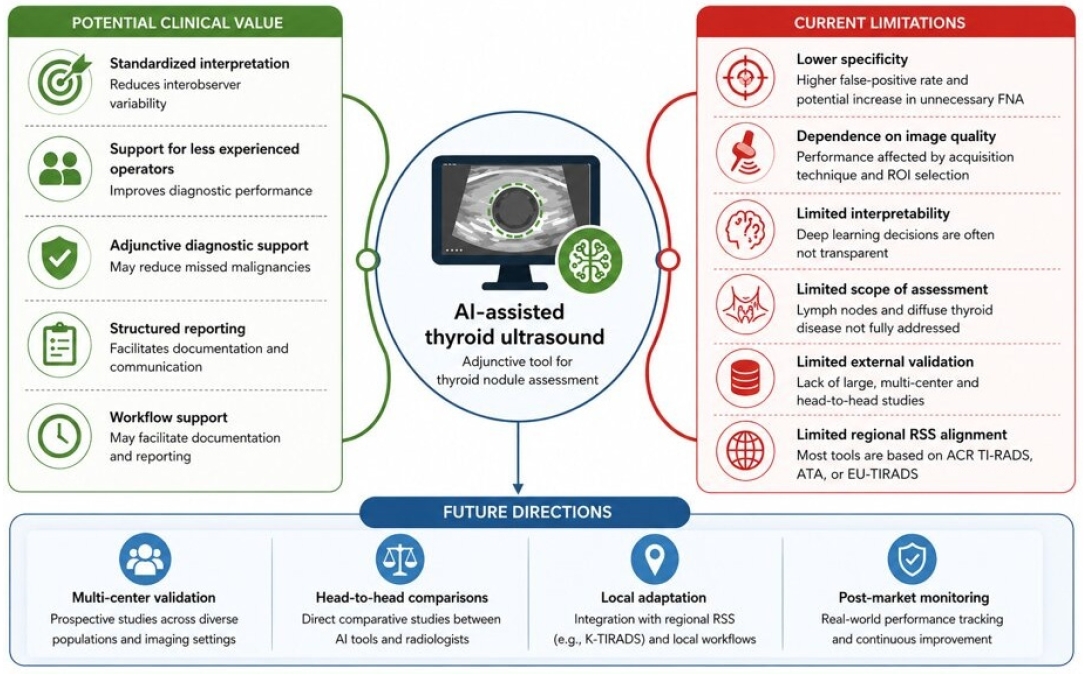
Clinical value, limitations, and future directions of AI tools for thyroid ultrasound. AI-assisted thyroid ultrasound may provide standardized interpretation, adjunctive diagnostic support, structured reporting, and workflow support, particularly for less experienced operators. Current limitations include lower specificity, dependence on image quality and ROI selection, limited interpretability, restricted assessment of lymph nodes and diffuse thyroid disease, limited external validation, and incomplete alignment with regional RSS. Future work should emphasize multi-center validation, head-to-head comparisons, local adaptation to regional RSS such as K-TIRADS, and post-market performance monitoring. AI, artificial intelligence; ROI, region of interest; RSS, risk stratification system; K-TIRADS, Korean Thyroid Imaging Reporting and Data System; FNA, fine-needle aspiration; ACR TI-RADS, American College of Radiology Thyroid Imaging Reporting and Data System; ATA, American Thyroid Association; EU-TIRADS, European Thyroid Imaging Reporting and Data System.
Development of Korean Thyroid Imagin Reporting and Data System-Integrated Artificial Intelligence Systems in Korea
Recognizing the limitations of currently available products, Korean researchers have pursued the development of AI tools specifically designed to integrate with K-TIRADS and the Korean clinical workflow. Kwak [11] reported on a domestically developed AI system (KH-UT1DAKR) that was trained on 4,750 thyroid US images (3,952 for training and 798 for validation) classified according to K-TIRADS criteria. Among several CNN architectures tested, the best-performing model (ResNet50d) achieved an overall accuracy of 90.6%, an AUC of 94.45%, a sensitivity of 82.14%, and a specificity of 95.17% [11].
This system features real-time integration with PACS, interactive ROI editing, automated K-TIRADS classification, and generation of structured screening reports, addressing many of the workflow integration gaps identified with currently available products [11]. These preliminary results are encouraging; however, direct comparison with cleared commercial tools is limited by differences in dataset composition, validation design, and clinical setting. Multi-center external validation will be necessary before definitive conclusions can be drawn regarding comparative performance.
Future Directions
Future studies should address several priorities. First, head-to-head comparisons of different AI products within the same patient cohort are needed. The current literature is limited by heterogeneous study designs that preclude direct cross-product comparison. Second, multi-center prospective trials across diverse clinical settings, including both academic centers and community practices, will be essential to establish the true incremental value of AI in everyday practice.
Third, the integration of AI with other data modalities warrants investigation. For example, combining US-based AI risk assessment with molecular markers from FNA samples could improve the management of cytologically indeterminate nodules, which represent a persistent diagnostic challenge [1]. AI has also been explored for lymph node assessment and for the evaluation of thyroid nodules incidentally discovered on computed tomography and magnetic resonance imaging [6,8].
Fourth, AI applications for automated report construction and clinical decision support have been described and may improve workflow efficiency and reduce reporting errors, though validation in diverse practice settings is required before clinical adoption [24].
Finally, the development of locally adapted AI systems, such as the K-TIRADS-integrated tool described by Kwak [11], underscores the importance of aligning AI products with regional clinical guidelines. For thyroid US, this issue is particularly relevant because biopsy thresholds and risk categories differ among ACR TI-RADS, EU-TIRADS, ATA guidelines, and K-TIRADS. In addition, prospective real-world validation after clinical implementation will be important to determine whether these tools improve diagnostic consistency, reduce unnecessary procedures, and maintain performance across different institutions, operators, and ultrasound equipment.
Conclusion
AI-based tools for thyroid nodule assessment on US have entered clinical practice as commercially available, regulatory-cleared products. As of early 2026, six such platforms have received FDA clearance. Most available studies suggest that these tools achieve sensitivity comparable to that of experienced radiologists and may improve the performance of less experienced operators. However, challenges remain in terms of specificity, workflow integration, interpretability, and alignment with regional classification systems such as K-TIRADS. Further multi-center validation, prospective real-world performance monitoring, and local adaptation to regional RSS are needed before these tools can be broadly in tegrated into routine thyroid US practice.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
All work was done by JWK.