Next-generation wearable neuromonitoring technologies: signal acquisition, modalities, and clinical relevance
Article information

Abstract
This narrative review, based on a non-systematic survey of the current literature, summarizes the current landscape of wearable neuromonitoring modalities—specifically high-density surface electromyography, in-ear electroencephalography, and flexible epidermal sensors. We outline their signal acquisition principles, technical advantages, and potential clinical relevance in scenarios such as postoperative spinal care, stroke neurorehabilitation, and Parkinson’s disease tracking. Furthermore, we discuss artificial intelligence as an emerging tool for processing high-dimensional wearable data, noting that many of these applications remain at an early or exploratory stage. Finally, we address key translational hurdles, including sensor biocompatibility and protocol standardization, that must be resolved to successfully integrate these wearable technologies into routine neurological assessment.
Introduction
The preservation and restoration of neural function represent primary goals in the management of neurological disorders and the surgical treatment of the central and peripheral nervous systems. Over the past few decades, intraoperative neuromonitoring (IONM)—incorporating modalities such as somatosensory evoked potentials, motor evoked potentials, and electromyography (EMG)—has enhanced surgical safety by providing real-time feedback on the functional integrity of neural pathways [1,2]. Despite its success in minimizing acute iatrogenic injuries, conventional IONM is fundamentally limited by its temporal boundaries; it ceases the moment the surgery concludes. Consequently, clinicians may still encounter delayed postoperative neurological deficits. These deficits often arise hours to days after surgery due to secondary pathophysiological mechanisms, including postoperative tissue edema, microvascular ischemia, or neuroinflammation, which occur long after the patient has left the highly monitored environment of the operating room [3-5].
Currently, the assessment of postoperative neural recovery or the progression of neurodegenerative diseases relies heavily on intermittent clinical evaluations and invasive neurophysiological testing, such as needle EMG and nerve conduction studies. While these tools possess high diagnostic accuracy, their invasive nature can inflict discomfort on patients, rendering them less suitable for continuous, longitudinal tracking [6,7]. Moreover, assessing a patient in a structured clinical setting may fail to capture the dynamic fluctuations of neural function that manifest during the activities of daily living. Phenomena such as motor fluctuations in Parkinson’s disease, stress-induced dysautonomia, or the complex corticomuscular interactions required for functional mobility post-stroke could benefit from sustained, real-world observation [8,9].
The evolution of materials science, microelectro-mechanical systems, and wireless telecommunications has catalyzed the emergence of wearable neuromonitoring technologies. By transitioning from rigid clinical machines to flexible, skin-conformable sensors, it is increasingly possible to monitor electroencephalography (EEG), EMG, and autonomic parameters in free-living environments [10-12]. Therefore, this review aims to highlight the intersection of these emerging wearable modalities and their clinical relevance. Rather than merely cataloging new devices, we examine how the technological foundations of high-density surface electromyography (HD-sEMG), in-ear EEG, and epidermal sensors may translate into sustained, real-world assessment strategies for postoperative care, neurorehabilitation, and movement disorder tracking. This article is structured as a narrative review; relevant literature was identified through targeted searches of PubMed, Scopus, and Google Scholar using key terms related to wearable neuromonitoring, surface EMG, in-ear EEG, and epidermal sensors. As this is not a systematic review, the selection of sources was guided by their relevance and recency rather than by a predefined protocol, and the conclusions drawn should be interpreted within this methodological context.
Pathophysiological Foundations of Continuous Neuromonitoring
To contextualize the development of wearable neuromonitoring technologies, it is helpful to briefly outline the temporal dynamics of nerve injury and neuroplasticity that necessitate continuous observation.
During spine or anterior neck surgeries, peripheral nerves and nerve roots may be subjected to mechanical forces such as traction or compression [13]. While acute severe trauma leads to immediate nerve disruption detectable by IONM, milder injuries often result in neurapraxia [14]. In the postoperative phase, localized tissue edema can increase interstitial pressure, leading to microvascular compression and delayed ischemia. Because these mechanisms evolve dynamically over several days, intermittent postoperative checks might miss the optimal therapeutic window [15]. In principle, continuous monitoring could detect early signs of motor unit irritability, such as subclinical fasciculations, which may in turn allowing for timelier clinical evaluation, although this application has not yet been validated in prospective clinical studies [16].
Similarly, in the central nervous system, recovery from conditions like stroke relies on neuroplasticity and cortical reorganization [17]. This process is highly activity-dependent and driven by the patient’s continuous interaction with their environment. While traditional neuroimaging captures brain activity in constrained moments, wearable tools have been proposed as a means to observe neuroplastic changes during real-world rehabilitation, though direct evidence for this capability remains limited [18]. Consequently, the dynamic nature of these physiological shifts necessitates the transition toward continuous, unobtrusive monitoring modalities.
Emerging Wearable Modalities for Neuromonitoring
The transition from clinical to wearable neuromonitoring requires overcoming significant biophysical challenges, primarily minimizing motion artifacts and maintaining stable sensor-skin interfaces. This section details three key modalities, focusing on their operational principles, technical characteristics, limitations, and potential applications.
1. High-density surface electromyography
Traditional bipolar surface EMG utilizes two electrodes to measure the global electrical activity of a muscle, which typically lacks spatial resolution and is susceptible to crosstalk [19]. In contrast, HD-sEMG deploys two-dimensional grids comprising tens to hundreds of miniaturized electrodes closely spaced (e.g., 3-8 mm apart). This configuration provides a high-resolution spatiotemporal map of the electrical potential distribution across the skin surface [20].
The primary technical advantage of HD-sEMG lies in its advanced signal processing capabilities. Utilizing mathematical algorithms such as blind source separation, the complex interference pattern recorded at the surface can be decomposed into the discharge trains of individual motor units [21]. This non-invasive extraction of motor unit action potentials and their firing rates mimics some of the diagnostic information traditionally obtained via invasive needle EMG [22].
Despite its potential, wearable HD-sEMG faces technical hurdles. The computational load required for real-time decomposition is substantial, challenging the battery life of wireless sensors. Additionally, maintaining uniform impedance across a large grid during dynamic movements remains difficult, as localized sweating or electrode lift-off can degrade signal quality.
In terms of exploratory applications, flexible HD-sEMG patches have been investigated for tracking physiological markers of reinnervation. As a damaged nerve regenerates, surviving motor neurons undergo collateral sprouting. Conceptually, by wearing an HD-sEMG array, a patient’s progressive reinnervation could be quantified over weeks, potentially serving as an objective biomarker for nerve regeneration speed, although clinical validation of this approach is still in its early stages [23].
2. In-ear electroencephalography
Prolonged cortical monitoring is often hampered by the obtrusiveness of conventional scalp EEG systems, which require wet gels and are prone to movement artifacts. In-ear EEG, often integrated into customized earpieces or "hearables," records electrical activity using dry or semi-dry electrodes placed directly within the ear canal or around the auricle [24].
Anatomically, the ear canal is in close proximity to the temporal lobes, providing a stable vantage point for recording auditory evoked potentials, sleep spindles, and certain epileptiform discharges. Because the ear canal is relatively stationary compared to the scalp and naturally holds the sensor securely, in-ear EEG tends to suppress motion artifacts and offers enhanced wearability for long-term daily use [25].
The most significant limitation of in-ear EEG is its low spatial resolution. Due to the small inter-electrode distance and confined anatomical location, it is generally unable to capture focal activities occurring in the frontal or occipital cortices. Furthermore, the limited number of channels restricts complex source localization.
Despite spatial constraints, in-ear EEG has shown preliminary utility in automated sleep staging, which is relevant since sleep architecture is often disrupted post-surgery and in neurodegenerative diseases. Furthermore, clinical studies have highlighted the inherent limitations of intraoperative monitoring in predicting delayed postoperative neurological events [10,16]. To help bridge this gap, it has been proposed that wearable EEG tracking could serve as an adjunctive tool to monitor postoperative arousal and neural network integrity in ambulatory environments, though this application remains largely conceptual at present.
3. Flexible epidermal sensors for autonomic monitoring
Autonomic nervous system dysfunction is a critical component of various conditions, ranging from systemic neuropathies to disorders of gut-brain interaction, where wearable monitoring is increasingly being evaluated [26]. Recent advancements in materials science have led to ultra-thin, flexible epidermal sensors designed specifically for continuous biomarker and autonomic tracking. Utilizing elastomeric substrates embedded with nanomaterials, these sensors exhibit mechanical properties that conform closely to the human epidermis.
For instance, epidermal wearable biosensors have been specifically engineered to continuously monitor biochemical markers in sweat, offering non-invasive tracking capabilities for chronic diseases [27]. Their thin profile makes them minimally obtrusive to the wearer, supporting high patient compliance in both clinical and home settings.
However, translating these devices to daily use requires overcoming mechanical limitations. Maintaining long-term durability necessitates robust, wireless, skin-integrated system designs that can function reliably across various physical healthcare environments [28].
From a neurophysiological perspective, integrating the continuous measurement of electrodermal activity and heart rate variability provides a direct window into assessing autonomic function and sympathovagal balance [29]. Consequently, this modality extends the reach of neuromonitoring beyond motor and sensory pathways, providing a potential window into stress-induced physiological changes and autonomic neuropathies.
Table 1 summarizes the key characteristics of the major wearable neuromonitoring modalities, including their signal acquisition principles, strengths, limitations, and representative clinical relevance.

Characteristics of emerging wearable neuromonitoring modalities
Representative Clinical Applications
While the technological capabilities of wearable sensors are expanding, their ultimate value lies in clinical translation. This section highlights representative clinical scenarios where these technologies could provide meaningful insights.
1. Postoperative care in spine and peripheral nerve surgery
Surgeries for cervical radiculopathy and myelopathy carry a risk of postoperative complications, such as C5 palsy, which typically manifests 2 to 7 days post-surgery. IONM has established the utility of tracking motor-evoked potentials to predict upper extremity motor paresis during such procedures [30,31]. Drawing upon these established IONM principles, it is conceivable that a wearable HD-sEMG array on the deltoid muscle could allow clinicians to extend motor unit recruitment monitoring into the postoperative ward. In this exploratory framework, observing a delayed drop in recruitment efficiency might alert the surgical team to impending neuropraxia. Similarly, building on the concepts of intraoperative recurrent laryngeal nerve assessment [32], wearable sensors placed on the neck could theoretically be used to track the postoperative recovery trajectory of vocal fold neuropraxia after thyroidectomy. It should be noted, however, that these postoperative applications have not yet been validated in controlled clinical trials and remain at a conceptual stage.
2. Neurorehabilitation and corticomuscular coherence
In stroke rehabilitation, assessing whether motor improvements stem from true neurological recovery or compensatory movements is challenging. Corticomuscular coherence (CMC) provides a mathematical measure of the functional coupling between the primary motor cortex (via EEG) and the contracting muscle (via EMG) [33]. By deploying a multimodal wearable system, clinicians could estimate CMC continuously during rehabilitative exercises. A progressive increase in beta-band CMC (15-30 Hz) over weeks of therapy has been hypothesized to reflect functional rewiring of the corticospinal tract, and could, if validated, serve as a digital biomarker to help time adjunct therapies such as robot-assisted training [34].
3. Tracking progression in neurodegenerative diseases
Optimizing dopaminergic medication in Parkinson’s disease requires an accurate understanding of the patient’s "On" and "Off" times, which typically relies on subjective patient diaries [8,11]. Wearable kinematics combined with surface EMG have been explored as an objective method to capture resting tremor characteristics, bradykinesia, and muscle rigidity under naturalistic conditions [35]. Over time, repeated sampling of these parameters can generate a personalized record of motor symptom fluctuations. While this continuous peripheral data is also being investigated for its potential to inform advanced closed-loop stimulation parameters [36], its primary near-term value lies in providing clinicians with an objective, continuous metric to guide routine medication adjustments.
Table 2 summarizes representative clinical scenarios in which wearable neuromonitoring technologies may provide meaningful longitudinal information beyond conventional intermittent assessment.
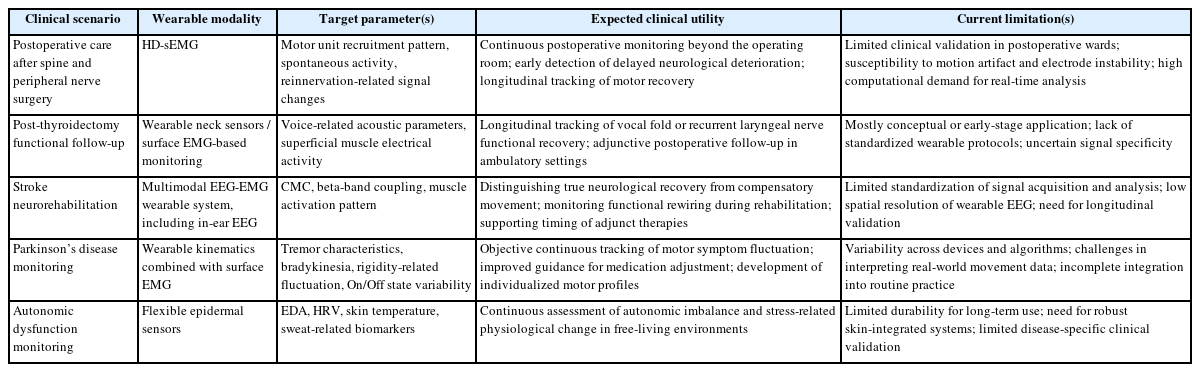
Representative clinical applications of wearable neuromonitoring technologies
Artificial Intelligence as an Enabling Tool
The integration of wearable continuous monitoring generates large volumes of high-dimensional data, rendering manual interpretation impractical. Consequently, artificial intelligence (AI) and machine learning (ML) are increasingly recognized as important enabling tools for signal processing and pattern recognition in this context, although their integration into wearable neuromonitoring workflows remains largely at the research and development stage.
1. Signal pre-processing and noise reduction
Real-world ambulatory data is inherently noisy and complex. AI algorithms, such as hybrid neural autoencoders, have been utilized to process and encode complex sensory and neural data efficiently [37]. In the context of wearable devices, the application of similar neural network architectures has the potential to assist in isolating physiological signals from background noise and baseline drift, which is a necessary step before any reliable clinical interpretation can occur. However, prospective validation of such pipelines on ambulatory wearable data remains limited.
2. Pattern recognition and prognostic assessment
Once the data is pre-processed, ML models can be utilized to handle the temporal dependencies of physiological time-series data. By analyzing extracted features, AI models may identify latent patterns related to patient mobility and neurological status. For instance, ML algorithms analyzing continuous gait parameters and wearable sensor data have demonstrated the ability to assess fall risk accurately among vulnerable populations [38,39]. Furthermore, AI methodologies have demonstrated robust capabilities in predicting severe neurological outcomes in critical care scenarios, such as post-cardiac resuscitation [40]. While originating from acute care, this illustrates the broader prognostic potential of AI in neurological monitoring; by applying similar pattern recognition frameworks to ambulatory wearable data, ML may in the future assist clinicians in stratifying patients based on objective digital biomarkers. At present, however, this translational step has not been broadly demonstrated, and further clinical studies are needed to establish the reliability and generalizability of such approaches.
Translational Challenges and Future Directions
Despite their potential, several critical translational hurdles remain to be resolved before wearable neuromonitoring achieves widespread clinical adoption.
Firstly, the biocompatibility and long-term durability of the sensor-skin interface require further refinement. Prolonged adhesion may cause skin irritation or signal degradation due to epidermal turnover and sweat accumulation. Continued research into breathable materials and stable conductive hydrogels is necessary to maintain low impedance without compromising patient comfort [23,28].
Secondly, rigorous clinical validation and standardization are urgently needed. Many current studies are proof-of-concept trials involving small cohorts. To establish wearable metrics as validated digital biomarkers, large-scale longitudinal trials are imperative. Additionally, standardizing data acquisition protocols, sensor placement, and feature extraction algorithms is essential to account for inter-individual variability in ambulatory settings [11,12].
Lastly, the continuous wireless transmission of neural data raises valid privacy and cybersecurity concerns. Robust encryption protocols and decentralized data processing techniques—where models are trained locally on the user’s device—should be further explored to safeguard patient data and comply with medical privacy regulations [11,18].
Table 3 outlines the major translational challenges that must be addressed before wearable neuromonitoring technologies can be implemented reliably in routine clinical practice.
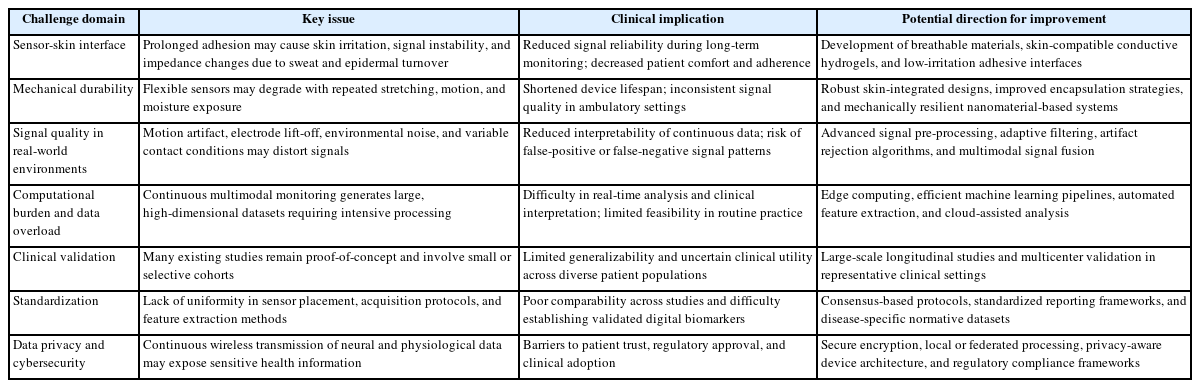
Translational challenges for the clinical implementation of wearable neuromonitoring technologies
Conclusion
The emergence of multimodal wearable neuromonitoring represents a notable technological advancement, offering the potential to shift certain aspects of neurological assessment from the clinic to the patient’s natural environment. By leveraging the signal acquisition capabilities of HD-sEMG, in-ear EEG, and flexible epidermal sensors, researchers and clinicians may eventually gain sustained, real-world insights into postoperative nerve recovery, corticomuscular neuroplasticity, and disease progression, provided that the current exploratory evidence is substantiated by rigorous clinical validation. As an enabling tool, AI provides the necessary framework to process these complex datasets. Overcoming the remaining translational hurdles, particularly regarding sensor durability, standardized clinical validation, and data security, will be crucial for translating these modalities into clinical practice, ultimately providing objective longitudinal tracking and adjunctive decision support.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
All work was done by PKJ.