
Introduction
Since Anuwong [1] reported the first clinical series of 60 transoral endoscopic thyroidectomy vestibular approach (TOETVA) cases in 2016, this technique has been rapidly adopted worldwide. Its primary advantage over other remote-access thyroidectomy approaches is the absence of a cutaneous scar, achieved through three mucosal incisions in the oral vestibule [2].
The safety profile of TOETVA has been examined in several pooled analyses. In a systematic review of the global literature through May 2020, Banuchi et al. [3] identified 1,880 unique TOETVA cases and reported pooled complication rates comparable to those of conventional transcervical thyroidectomy, including hematoma (0.4%), transient recurrent laryngeal nerve (RLN) palsy (3.9%), permanent RLN palsy (0.6%), transient hypoparathyroidism (16.8%), permanent hypoparathyroidism (0.9%), and infection (1.1%). Wang et al. [4]’s meta-analysis of 478 TOETVA and 673 transcervical patients found no significant differences in RLN palsy, hypocalcemia, or hematoma between the two approaches. de Vries et al. [5]’s broader systematic review of minimally invasive thyroidectomy techniques, encompassing 736 TOETVA patients, similarly reported a comparable temporary RLN palsy rate of 4.0% for TOETVA versus 3.3% for open thyroidectomy.
However, TOETVA introduces complications that are unique to the transoral route. Among these, mental nerve injury, manifesting as numbness or paresthesia of the chin and lower lip, is one of the most frequently discussed [6]. The reported incidence is remarkably variable, ranging from 0% in some series to over 80% in others [6,7]. This wide range likely reflects both true technical differences (port placement, surgeon experience, learning curve) and methodological differences in outcome assessment (definitions of "injury," measurement tools, follow-up duration) [6,8].
Three interrelated lines of investigation have begun to address this issue. The first is cadaveric anatomical work defining a midline safety zone free of mental nerve branches. The second is prospective clinical measurement of postoperative sensory changes using standardized instruments. The third is technical modifications, including gasless single-incision approaches, designed to minimize vestibular dissection and nerve traction. The present review synthesizes these three lines of evidence, with particular emphasis on the anatomical study by Yang et al. [9] and the prospective clinical series by Woo et al. [10]. It is important to note at the outset that the current evidence base is limited in both volume and diversity: these core studies originate from a small group of investigators, and the broader literature on mental nerve outcomes after TOETVA is characterized by marked heterogeneity in patient populations, surgical techniques, and outcome definitions. Caution is therefore warranted in generalizing any single set of findings. Table 1 summarizes the key studies addressing the anatomical basis, postoperative sensory outcomes, and technical modifications related to mental nerve preservation in TOETVA.
Anatomical Basis for the Midline Safety Zone
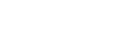
Understanding the branching pattern of the mental nerve is essential for safe port placement in transoral thyroidectomy. The mental nerve emerges from the mental foramen of the mandible, typically below the second premolar, and divides into three to four terminal branches supplying sensation to the chin and lower lip [11]. Several cadaveric studies have investigated the surgical anatomy of this nerve in the context of TOETVA [6,8,11]. The anatomical rationale for a midline lower-risk corridor in TOETVA is summarized in Figure 1, which depicts the mental nerve course, inferior labial branches, and the proposed central vestibular safety zone in relation to recommended incision and port placement.
The most detailed mapping to date was reported by Yang et al. [9], who applied modified Sihler’s whole-nerve staining to 20 unilateral cadaveric specimens. This technique renders surrounding soft tissue transparent while preserving nerve fibers intact, enabling visualization of the full arborization pattern without the distortion inherent to conventional dissection. The inferior labial branches were found to fan out from the mental nerve trunk across the lower lip, with the most lateral branch reaching close to the oral commissure, while a nerve-free zone was consistently present in the medial region. Based on these observations, the authors proposed a trapezoidal safety zone in the central oral vestibule, approximately 3 cm wide at its base, within which a midline incision and instrument insertion could be performed with reduced risk of direct nerve transection.
Other investigators have provided complementary data. King et al. [8] described eight distinct branching patterns of the mental nerve based on 120 cadaveric dissections and recommended placing lateral vestibular incisions at least 3-3.5 cm from the midline, lateral to the mental foramen. Zhang et al. [12] reported that a 10-mm midline vestibular incision placed at a high level near the lip vermilion could transect medial inferior labial branches in 12%-25% of cases, recommending a more inferior or vertical incision. These findings collectively support the principle that the central vestibular region represents the lowest-risk corridor for transoral access, but also indicate that anatomical variation exists and no zone can be considered universally safe.
For practicing surgeons, the practical takeaway from this anatomical literature is twofold: the central incision should be placed at the base of the lower lip frenulum rather than near the vermilion, and lateral ports should be positioned as close as possible to the oral commissure. However, cadaveric studies cannot replicate the mechanical stresses of trocar insertion and instrument manipulation in a living patient, and sample sizes to date have been modest. Additional anatomical studies with larger and ethnically diverse cohorts would strengthen these recommendations.
Clinical Evidence: Sensory Outcomes After Transoral Thyroidectomy
1. The challenge of measurement heterogeneity
Before examining specific studies, it is worth emphasizing that the single greatest obstacle to synthesizing the mental nerve injury literature is the absence of a consensus definition and standardized assessment protocol. Some studies define injury as any subjective alteration reported by the patient, while others require objective demonstration of elevated pressure thresholds or loss of two-point discrimination [6]. Still others use composite scoring systems or focus solely on persistent deficits beyond an arbitrary time cutoff. This heterogeneity makes direct comparison across series difficult and partly explains the wide range of reported incidence rates (0%-81%). Any interpretation of specific studies must be read against this background.
2. Threshold-based monofilament studies
Among the earliest objective evaluations, Tae et al. [13] applied the Semmes-Weinstein monofilament test to 10 cutaneous zones in 43 patients undergoing transoral robotic or endoscopic thyroidectomy. Chin and lower-lip pressure thresholds remained unchanged postoperatively, while the submental and level VI regions showed transient threshold elevations that normalized within 3 months. The authors interpreted these findings as evidence that the mental nerve is adequately preserved when vestibular incisions are properly placed. From a methodological standpoint, however, threshold testing at predetermined points may not capture focal or spatially distributed sensory changes that fall below the detection threshold at any individual site, a limitation that later studies sought to address with area-based mapping.
At the other extreme, Zheng et al. [7] documented varying degrees of mental nerve paraesthesia in 81.1% of 297 patients, with permanent paraesthesia in seven cases (2.4%). The difference between these two studies (0% versus 81% reported mental nerve paraesthesia rates) illustrates how profoundly the choice of assessment method and definition of "injury" can influence reported outcomes.
3. Area-based monofilament mapping
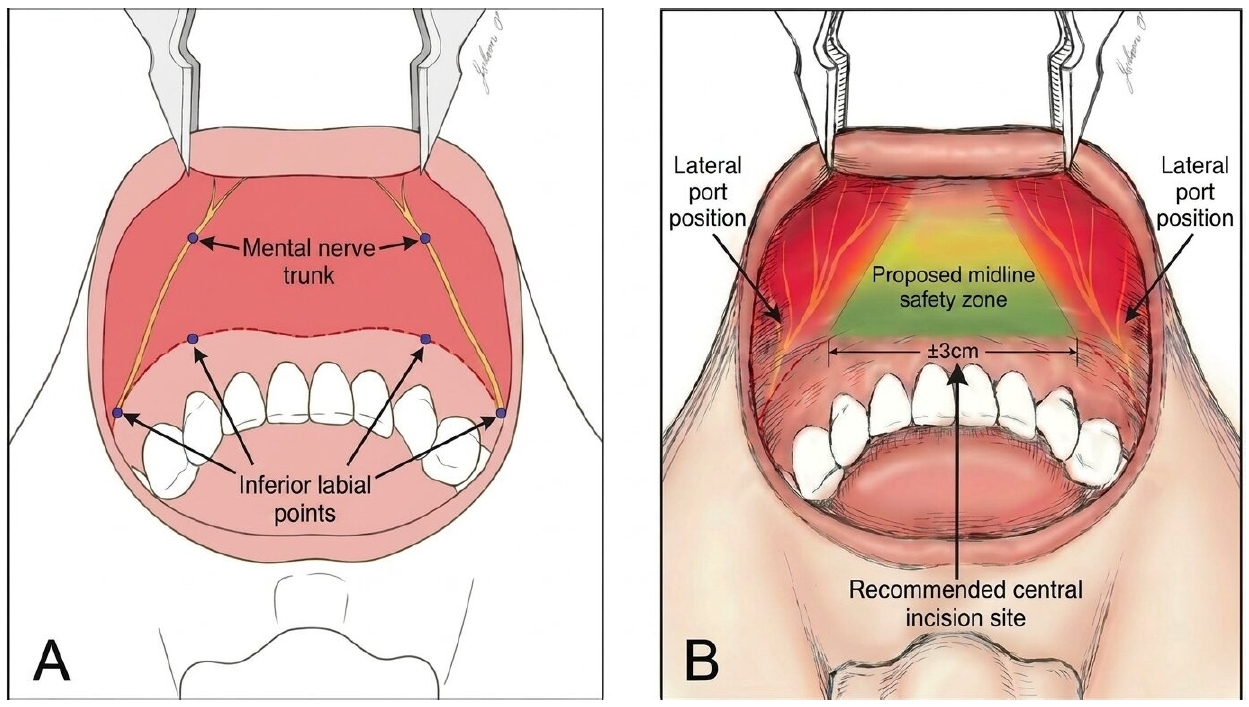
A different methodological approach was taken by Woo et al. [10], who quantified postoperative sensory deficit as a mapped area (mm2) rather than a threshold value at fixed points. In their prospective cohort of 37 gasless transoral and 40 conventional thyroidectomy patients, all of whom proved to have papillary thyroid carcinoma on final pathology, area-based monofilament mapping revealed universal early sensory loss in the transoral group. It should be noted that this finding was detected by a highly sensitive spatial mapping technique, and the measured deficits may not necessarily correspond to clinically significant patient-reported morbidity. The mean deficit area was large at 1 week (535 mm2), contracted substantially by 1 month (115 mm2), and approached near-resolution by 2 months (21 mm2; p=0.028), with five patients (13.5%) achieving complete recovery within that period. No measurable deficit occurred in the conventional-surgery controls at any time point.
Two features of the data merit comment in the context of the broader literature. First, the remarkably narrow variability at 1 week relative to the mean suggests that early sensory loss is a near-uniform consequence of the transoral approach itself, rather than an outlier event. Second, the progressively wider relative variability at later time points reflects diverging individual recovery trajectories, a pattern consistent with neuropraxia of varying severity rather than a single uniform mechanism. Figure 2 summarizes the postoperative course, showing both the quantitative reduction in deficit area and the representative spatial pattern of centripetal recovery.
The observation that sensory loss occurred uniformly despite adherence to the anatomically defined safety zone is noteworthy because it implies that direct nerve transection is not the sole, or even the primary, mechanism. Mechanical traction during flap elevation and retractor placement offers a plausible alternative explanation, and the centripetal pattern of recovery reported by Woo et al. [10] is broadly consistent with gradual resolution of conduction block. However, the precise pathophysiology cannot be inferred from clinical mapping data alone, and prospective studies incorporating electrophysiological testing would be needed to distinguish neuropraxia from other mechanisms such as perineural edema or microvascular compromise.
4. Integrating the evidence
Viewed collectively, the available studies delineate a spectrum of postoperative sensory change that is highly dependent on how and when sensation is measured. Threshold-based testing at fixed points, as used by Tae et al. [13], may classify most patients as unaffected, whereas area-based mapping, as employed by Woo et al. [10], detects near-universal early deficits. Neither approach is inherently superior; rather, they capture different dimensions of sensory function. The clinical significance of minor, transient changes remains debatable, and true permanent injury, defined as persistent sensory loss beyond 6 to 12 months, appears to be uncommon when established technical principles are followed. Several limitations constrain the strength of these conclusions. Both the Tae et al. [13] and Woo et al. [10] studies originate from Korean centers with collaborative ties, and neither has been independently replicated in geographically or institutionally diverse settings. Sample sizes are modest, follow-up in the Woo et al. [10] cohort extends only to 2 months, and the gasless single-incision technique used by Woo et al. [10] differs from the standard three-port CO2-insufflated TOETVA evaluated in most other series, limiting direct comparability. For surgeons interpreting these data, the practical implication is that some degree of early sensory disturbance likely represents a common accompaniment of the transoral approach rather than an indication of surgical error, provided it follows the expected trajectory of progressive resolution.
Technical Modifications Relevant to Mental Nerve Preservation
1. Port placement and incision design
Since the original TOETVA technique was introduced, several modifications to port placement have been proposed to reduce mental nerve risk. Anuwong’s initial series [1] placed the two lateral 5-mm ports relatively close to the midline. Subsequent experience demonstrated that moving these incisions laterally, toward the oral commissure, reduced the incidence of mental nerve disturbance and improved instrument triangulation [2,6]. In a narrative review, Wolfe and Russell [14] proposed an arc-shaped middle mucosal incision combined with lateral incisions near the oral commissure adjacent to the mucosal folds, reporting a significant reduction in time to sensory recovery (1.9 months vs. 4.5 months, p˂ 0.001) and in the proportion of patients with sensory alterations immediately postoperatively (79.5% vs. 100%) compared with the original incision design. However, the original study was published in a non-English journal, and the data should be interpreted with this limitation in mind.
2. Gasless single-incision approach
The standard TOETVA technique employs CO2 insufflation at 6 mmHg to maintain the working space. While this pressure is relatively low, CO2-related complications, including embolism, subcutaneous emphysema, and hypercapnia, have been reported [6,15]. In the clinical arm of the same study, Yang et al. [9] compared 31 gasless transoral thyroidectomies with 31 conventional transcervical procedures in patients with predominantly benign thyroid disease. Complication profiles were comparable between groups, and no mental nerve injury was clinically detected in either cohort. Operative times, however, were significantly longer for the transoral approach (90.2 minutes vs. 61.2 minutes, p=0.001), a difference the authors attributed largely to the learning curve of the endoscope assistant rather than intrinsic technical complexity.
The theoretical advantage of the gasless single-incision approach for mental nerve preservation lies in its confinement of all vestibular dissection to the midline safety zone, avoiding lateral port sites that are closest to the mental nerve branches. Notably, this absence of clinically detected mental nerve injury should be interpreted with caution, as the study was not specifically designed to assess sensory outcomes with quantitative instruments such as monofilament mapping. By eliminating CO2 insufflation, it also removes the risk of gas embolism. However, no randomized comparative study has directly evaluated mental nerve outcomes between gasless single-incision technique and standard three-port TOETVA. The authors noted that the most time-consuming element was adaptation of the endoscope assistant to the transoral approach, suggesting that operative times may decrease with experience. For the moment, this approach represents a conceptually attractive modification, but its potential benefit for mental nerve preservation remains entirely theoretical until direct comparative studies employing standardized quantitative sensory testing are available.
Implications for Practice
The evidence reviewed here supports several practical considerations, each tempered by the limitations of the available data.
Preoperative counseling for patients considering transoral thyroidectomy should explicitly address the high likelihood of transient chin and lower-lip sensory disturbance. Based on the available prospective data, patients can be informed that the affected area typically decreases substantially within 1 to 2 months, though a minority may have residual minor changes beyond this period. The cosmetic benefit of a scarless approach should be weighed against this temporary sensory trade-off on an individual basis, with the understanding that complete long-term data remain limited.
Regarding surgical technique, strict adherence to the anatomically defined midline safety zone during vestibular incision and dissection is the best-supported strategy for minimizing the risk of direct mental nerve injury. Lateral ports should be placed near the oral commissure, and the central incision should be at the base of the lower lip frenulum rather than near the vermilion. Whether the gasless single-incision approach offers a clinically meaningful additional advantage over well-placed three-port TOETVA with respect to nerve outcomes awaits direct comparative evidence.
The wide variation in reported mental nerve injury rates underscores the need for a consensus definition and standardized assessment protocol. Area-based monofilament mapping, as employed by Woo et al. [10], offers a more granular and quantitative measure than binary subjective reporting or threshold-based testing at fixed points. If adopted across centers, such a method could facilitate meaningful outcome comparisons and help distinguish clinically significant injury from the expected transient sensory changes. Table 2 provides a practical summary of anatomy-based surgical considerations and postoperative counseling points relevant to mental nerve-related sensory change after TOETVA.
Conclusion
Transoral endoscopic thyroidectomy offers a cosmetically superior alternative to conventional cervical thyroidectomy. Mental nerve sensory disturbance appears to be largely transient when surgery is performed within the anatomically defined midline safety zone, though the current evidence base remains limited by small sample sizes, short follow-up, and measurement heterogeneity. Multicenter studies with standardized sensory outcome measures and longer follow-up are needed to establish the true incidence, natural history, and optimal technical approach. Until such data are available, clinicians may reasonably regard early postoperative sensory change as a generally self-limiting accompaniment of the transoral approach. Patient counseling should clearly distinguish between this expected transient sensory change and true persistent mental nerve injury, which remains uncommon when established technical principles are followed.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




