Single-port transaxillary robotic thyroidectomy and lateral neck dissection: technique, early outcomes, and neuromonitoring
Article information

Abstract
Therapeutic lateral neck dissection is recommended for papillary thyroid carcinoma with clinically evident lateral cervical lymph node metastasis (N1b). Conventional open surgery provides reliable oncologic outcomes but leaves a cervical scar. Remote-access robotic surgery was introduced to avoid a visible neck incision, with subsequent studies reporting comparable lymph node yields. The da Vinci single-port (SP) system delivers wristed instruments and a flexible three-dimensional endoscope through a single 2.5-cm cannula. Early clinical series from experienced Korean centers have reported lateral lymph node yields and short-term complication rates comparable to those of multiport robotic and open approaches, though operative time was initially longer. Intraoperative neuromonitoring (IONM) using the V1-R1-R2-V2 protocol may facilitate recurrent laryngeal nerve identification and functional assessment, while extended stimulation may aid assessment of the spinal accessory and phrenic nerves during lateral neck dissection. However, current evidence remains limited to small, predominantly single-center retrospective series, and no SP-specific IONM outcome data are currently available. Prospective multicenter studies with long-term oncologic follow-up are needed before broader adoption of this technique can be recommended.
Introduction
Clinically evident lateral cervical lymph node metastasis is less frequent than central compartment disease in papillary thyroid carcinoma (PTC), but it carries important surgical implications. The 2015 and 2025 American Thyroid Association (ATA) guidelines recommend therapeutic lateral neck dissection for biopsy-proven N1b disease, while the 2012 ATA surgical affairs committee consensus statement clarifies the typical compartment-oriented extent, including levels IIa, III, IV, and Vb [1-3].
Open modified radical neck dissection (MRND) remains the standard approach. While it affords direct access and well-documented long-term oncologic safety, it produces a transverse cervical incision that may negatively affect patient satisfaction with neck appearance. Kim et al. [4] demonstrated in a multicenter randomized controlled trial that cervical scar outcomes after conventional thyroidectomy are measurably affected by wound management technique, underscoring the cosmetic relevance of surgical access.
Remote-access surgery was introduced as a way to avoid a visible cervical incision while maintaining access to the central and lateral neck compartments. Kang et al. [5] reported the first large series of robotic transaxillary thyroidectomy using the da Vinci system in 2009, and by 2022, Kim et al. [6] had accumulated experience with robotic transaxillary lateral neck dissection in over 500 patients. Meanwhile, bilateral axillo-breast approach (BABA) robotic MRND was reported by Choi and Kang [7] in 2017. The da Vinci single-port (SP) system was later adapted for transaxillary thyroidectomy and, subsequently, lateral neck dissection.
This narrative review examines the current evidence on SP transaxillary robotic lateral neck dissection using the da Vinci SP system, describes the published surgical techniques, and discusses the role of intraoperative neuromonitoring (IONM) in this setting.
The da Vinci Single-Port System: Technical Features and Regulatory Status
The SP platform is distinguished by its single-cannula configuration [8,9]. Three semi-rigid, fully wristed instruments and a flexible three-dimensional high-definition endoscope are introduced through one 2.5-cm cannula (Intuitive Surgical, Inc.). Each instrument arm has multiple joints that enable triangulation within the operative field, and the endoscope itself is fully articulated, allowing the surgeon to adjust the viewing angle independently of the instruments. The “relocation” function permits repositioning of the instrument cluster toward a new target zone within the same operative field, which is particularly useful when transitioning from thyroidectomy to lateral neck dissection.
The da Vinci SP system received initial U.S. Food and Drug Administration (FDA) 510(k) clearance for SP urologic surgical procedures in May 2018 (K173906) [8]. In March 2019, a supplemental clearance (K182371) expanded the indications to include transoral otolaryngology surgical procedures in the oropharynx, restricted to benign tumors and malignant tumors classified as T1 and T2 [9]. Intuitive Surgical issued a press release describing this transoral clearance [10]. Both clearance documents state that safety and effectiveness for general laparoscopic procedures have not been established [8,9]. Transaxillary thyroidectomy and lateral neck dissection are not among the FDA-cleared indications, and their use with the SP system therefore constitutes off-label application.
The current SP platform also has practical limitations. In the published SP thyroid and neck dissection series, the lack of a robotic ultrasonic energy device for the SP cannula has been cited as a practical limitation; surgeons may rely on monopolar and bipolar energy or use conventional energy instruments through an auxiliary port. Counter-traction depends on assistant-held instruments introduced through an auxiliary port. Workspace constraints may be encountered during dissection of level IV near the clavicle, and, in gas-insufflation approaches, CO2 management requires additional attention. The technical characteristics, regulatory status, and practical limitations of the da Vinci SP system in transaxillary thyroid and lateral neck surgery are summarized in Table 1.
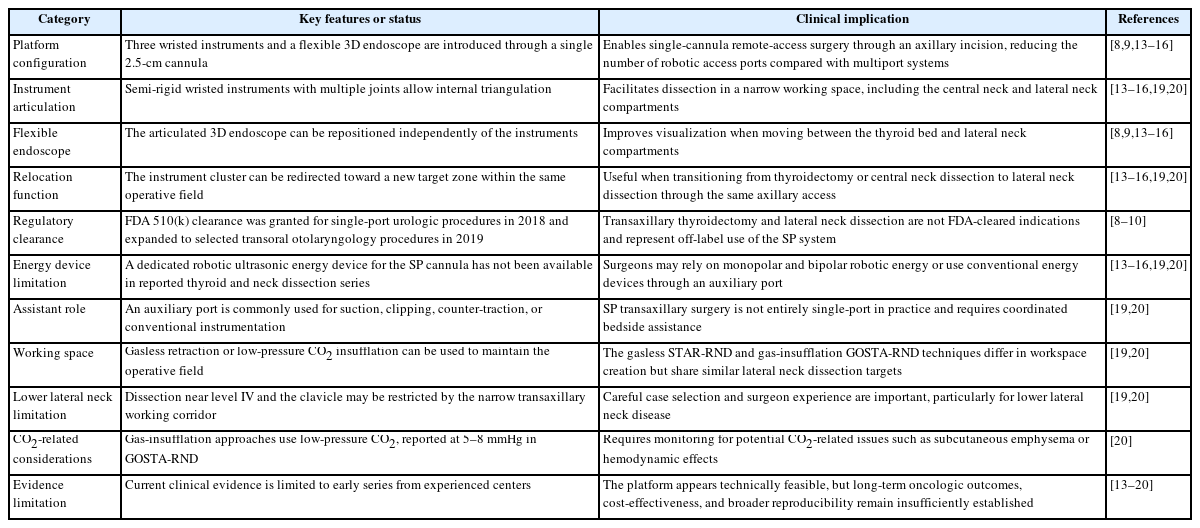
Key features and limitations of the da Vinci SP system in transaxillary thyroid and lateral neck surgery
Evolution of Robotic Approaches to Lateral Neck Dissection
Robotic transaxillary thyroidectomy was first applied clinically by Kang et al. [5] in 2007, and the initial 100-case series was published in 2009. Extension of the transaxillary approach to lateral neck compartments followed, with Kang and Chung [11] reporting the first robotic MRND in 2015. Kim et al. [12] subsequently published a 5-year comparative assessment of transaxillary robotic versus open MRND in 193 N1b PTC patients, demonstrating comparable recurrence rates and stimulated thyroglobulin levels over a median follow-up of 66 months.
In a 500-case series, robotic transaxillary lateral neck dissection was completed without open conversion and showed acceptable operative and oncologic outcomes in a high-volume center [6]. This multiport experience supported the feasibility of comprehensive lateral compartment dissection through a remote-access route and laid the groundwork for subsequent SP applications.
The SP platform was first applied to transaxillary hemithyroidectomy by Kim et al. [13] in 2020, and the experience was subsequently expanded to larger thyroidectomy series, providing the technical foundation for SP lateral neck dissection [14-16]. Park et al. [16] reported a learning curve of approximately 20 cases for SP transaxillary lobectomy in surgeons with prior robotic experience. Kim [17] provided a comprehensive review of the evolution and clinical impact of SP transaxillary robotic thyroidectomy in 2025. Experience with SP robotic areolar-MRND remains limited to a single small series, whereas the transaxillary approach has relatively more clinical data [18]. The evolution of robotic approaches to lateral neck dissection and the current position of SP transaxillary robotic lateral neck dissection are summarized in Table 2.
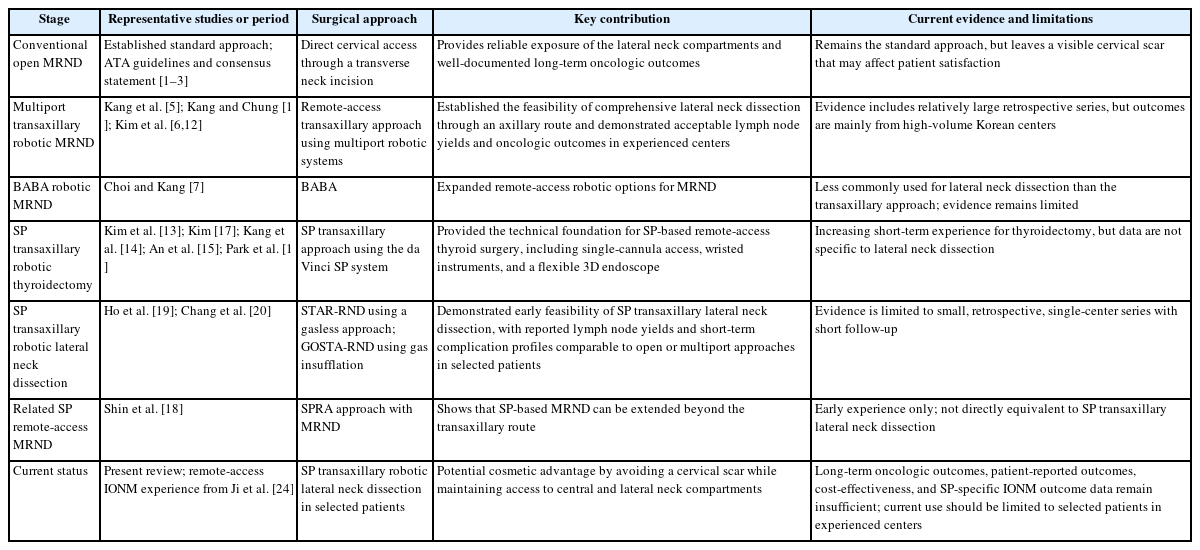
Evolution of robotic lateral neck dissection approaches
Surgical Technique for Single-Port Transaxillary Lateral Neck Dissection
The published SP transaxillary MRND techniques can be broadly divided into gasless and gas-insufflation approaches.
1. STAR-RND (gasless approach)
Ho et al. [19] described a gasless technique using an axillary skin incision (4-6 cm), through which a subcutaneous and subplatysmal flap is elevated over the sternocleidomastoid muscle to the lateral neck. An external retractor system maintains the working space. The SP cannula is introduced through the axillary incision, and dissection proceeds in a caudal-to-cranial sequence: level IV and Vb first, then level III, and finally level IIa and IIb. The spinal accessory and phrenic nerves are identified during lateral neck dissection, while the vagus nerve and recurrent laryngeal nerve (RLN) are assessed during thyroidectomy and central neck dissection when performed concurrently. An auxiliary 5-mm trocar accommodates suction and clip applier instruments controlled by the bedside assistant. When thyroidectomy is performed concurrently, the same axillary access is used, and the relocation function allows the instrument cluster to be shifted medially [19].
2. GOSTA-RND (gas-insufflation approach)
Chang et al. [20] described a gas-insufflation one-step SP transaxillary approach in which a glove port is used to create a sealed access through the axillary incision. Low-pressure CO2 insufflation (5-8 mmHg) is applied to maintain the operative space. The dissection sequence and anatomic targets are similar to those of the STAR-RND (single-port transaxillary robotic neck dissection). The gas-insufflation technique may reduce the need for external retraction and provide a more stable operative field, though CO2-related considerations (subcutaneous emphysema, hemodynamic effects) require monitoring [20].
In both approaches, the articulating SP instruments are used to dissect the lateral neck through a remote axillary access. Both employ a bedside assistant for tasks that cannot be performed robotically.
Early Clinical Outcomes of Single-Port Transaxillary Lateral Neck Dissection
In the STAR-RND series of 30 patients, mean lateral lymph node yield was 34.6, with no permanent nerve injury, hypoparathyroidism, or major vascular injury [19]. In the GOSTA-RND (gas-insufflation one-step single-port transaxillary robotic neck dissection) comparative series (30 robotic vs. 39 open), lateral lymph node yields and complication profiles were similar, though early robotic cases required longer operative time [20]. With increasing experience, operative time for the lateral dissection component was reported to decrease substantially.
At present, published clinical data on SP-based lateral neck dissection are limited to these early series. Although the short-term results suggest feasibility, several limitations remain. All data come from single Korean centers with extensive prior robotic thyroid surgery experience. Patient cohorts are small and retrospectively analyzed. Follow-up is insufficient to draw conclusions about long-term recurrence rates or disease-specific survival. Selection criteria generally favor patients with favorable body habitus and limited disease burden. Therefore, SP transaxillary lateral neck dissection should currently be limited to carefully selected patients and performed in experienced centers with substantial expertise in robotic thyroid surgery. The findings should be interpreted as evidence of technical feasibility and early safety rather than definitive proof of oncologic equivalence. Published clinical evidence on SP robotic thyroidectomy, SP transaxillary lateral neck dissection, and remote-access IONM is summarized in Table 3.
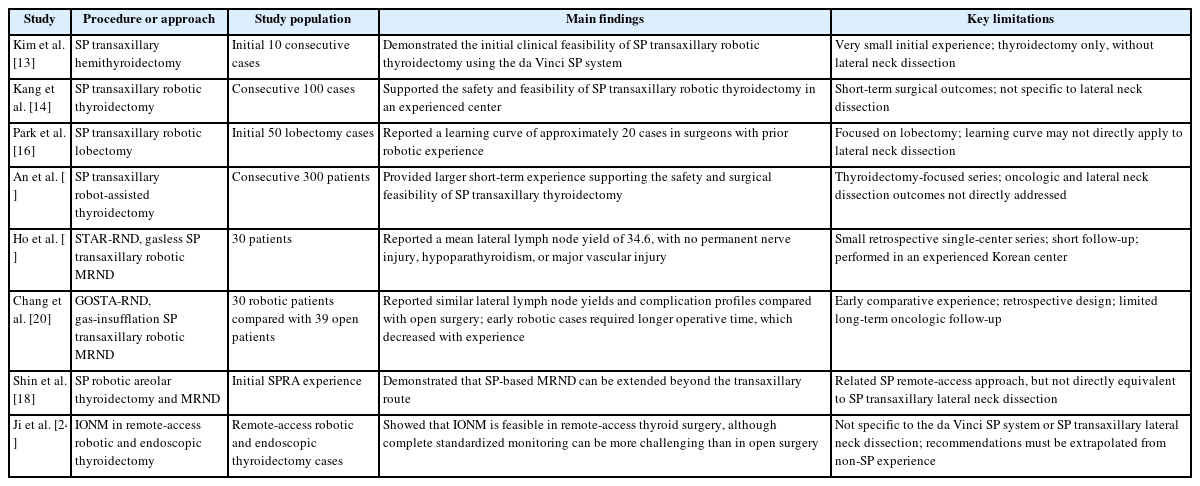
Published clinical evidence on SP robotic thyroidectomy and lateral neck dissection
Intraoperative Neuromonitoring in Robotic Lateral Neck Dissection
In robotic lateral neck dissection, neural preservation is a central technical concern. The confined, remote operative field and the absence of direct tactile feedback make visual identification of nerves more challenging than in open surgery. IONM provides an adjunctive means of confirming nerve identity and assessing functional status during dissection.
The standard IONM protocol (V1-R1-R2-V2) was originally developed and validated for RLN monitoring during open thyroidectomy [21]. In this protocol, the vagus nerve is stimulated before (V1) and after (V2) thyroid resection, and the RLN is stimulated before (R1) and after (R2) lobectomy, with electromyographic (EMG) signals recorded from the vocalis muscle via an endotracheal tube electrode. A recent systematic review suggests that IONM has high specificity for predicting postoperative vocal cord palsy, though its impact on the rate of permanent nerve injury remains debated [22].
Extension of IONM to the lateral neck permits monitoring of the spinal accessory nerve (SAN) and phrenic nerve in addition to the RLN and vagus nerve. In open MRND, SAN monitoring has been shown to be technically feasible and may reduce the incidence of postoperative shoulder dysfunction [23]. During robotic lateral neck dissection, IONM electrodes for the RLN are placed via the endotracheal tube as in open surgery, while SAN monitoring can be achieved using surface electrodes on the trapezius muscle. Figure 1 summarizes the surgical access, lateral neck dissection sequence, and neuromonitoring targets for SP transaxillary robotic lateral neck dissection.
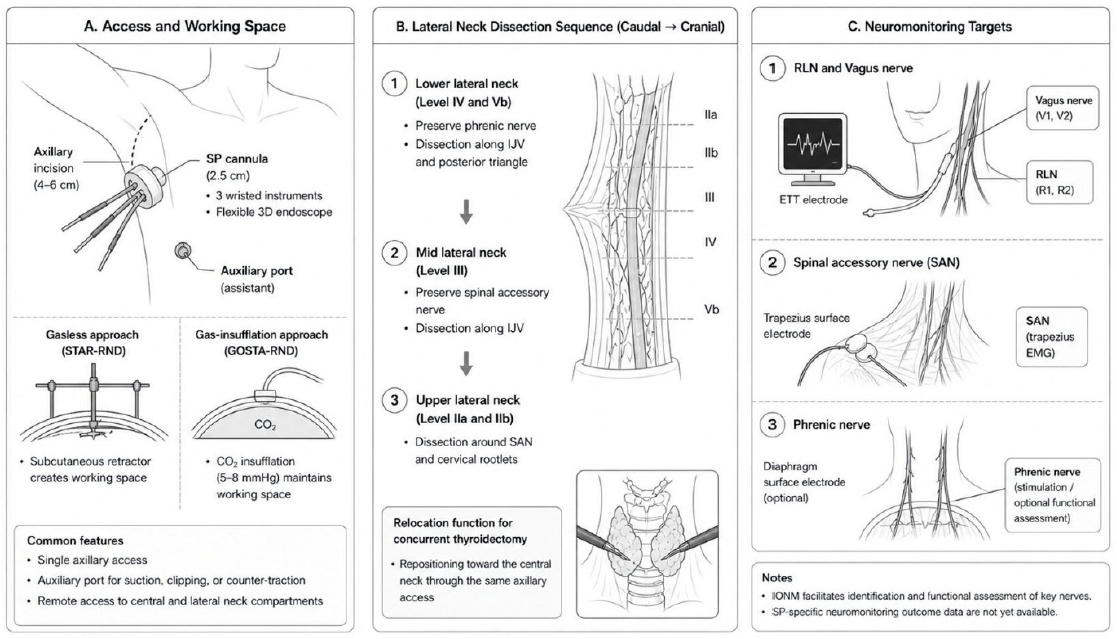
Surgical concept and neuromonitoring targets in SP transaxillary robotic lateral neck dissection. (A) The SP transaxillary approach uses a single axillary incision for introduction of the SP cannula, with an auxiliary port used for suction, clipping, or counter-traction. The operative space may be created using a gasless retractor system, as in STAR-RND, or maintained using low-pressure CO2 insufflation, as in GOSTA-RND. (B) Lateral neck dissection is generally performed in a caudal-to-cranial sequence, beginning with the lower lateral neck, including levels IV and Vb, followed by level III and then the upper lateral neck, including levels IIa and IIb. When thyroidectomy is performed concurrently, the SP relocation function allows repositioning toward the central neck through the same axillary access. (C) Neuromonitoring may include standard V1-R1-R2-V2 monitoring of the vagus nerve and RLN using an ETT electrode, as well as extended monitoring of the SAN using trapezius surface electrodes. Phrenic nerve stimulation or optional functional assessment may be considered during lower lateral neck dissection, although standardized SP-specific neuromonitoring protocols and outcome data are not yet available. SP, single-port; 3D, three-dimensional; GOSTA-RND, gas-insufflation one-step single-port transaxillary robotic neck dissection; STAR-RND, single-port transaxillary robotic neck dissection; IJV, internal jugular vein; RLN, recurrent laryngeal nerve; EMG, electromyography; ETT, endotracheal tube; IONM, intraoperative neuromonitoring.
Ji et al. [24] reported on the feasibility and efficacy of IONM in remote-access robotic and endoscopic thyroidectomy, observing that complete standardized monitoring was more challenging than in open surgery, particularly during the early experience with transoral approaches. Continuous IONM, which provides real-time EMG feedback during dissection rather than intermittent stimulation, has been investigated in open thyroidectomy and may offer earlier detection of impending nerve injury from traction or compression. Its application in robotic surgery remains limited by the need for a vagal electrode and the additional operative complexity.
No SP-specific IONM outcome data have been published to date. Therefore, current recommendations for neuromonitoring in SP transaxillary robotic lateral neck dissection are extrapolated from open thyroidectomy, open lateral neck dissection, and multiport remote-access robotic surgery. Although these principles are likely applicable, the narrower instrument corridor and single-cannula access may affect electrode placement and stimulation angles. Future work may also explore improved integration of EMG feedback into the robotic console, although this remains a technical goal rather than an established clinical tool.
Conclusion
SP transaxillary robotic lateral neck dissection using the da Vinci SP system is technically achievable, but it should currently be reserved for carefully selected patients in experienced centers. Early series demonstrate lateral lymph node yields and short-term complication rates comparable to those of multiport robotic and open MRND, with the advantage of avoiding a cervical scar. However, the evidence base remains limited to small, retrospective, single-center Korean series with short follow-up, and the results should be interpreted with caution.
IONM is a valuable adjunct for nerve identification during robotic lateral neck dissection, although SP-specific outcome data are not yet available and its specific contribution to reducing permanent nerve injury in this setting has not been established. Standardized IONM protocols adapted for SP robotic access warrant further development.
Prospective multicenter studies with long-term oncologic follow-up, patient-reported outcomes, and cost-effectiveness analyses are needed before broader adoption of SP transaxillary robotic lateral neck dissection can be recommended.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
All work was done by KK.