
Introduction
Intraoperative neuromonitoring (IONM) has been widely adopted during thyroid and parathyroid surgery, providing real-time functional assessment of the recurrent laryngeal nerve (RLN) and the external branch of the superior laryngeal nerve (EBSLN) [1,2]. The International Neural Monitoring Study Group (INMSG) established a standardized four-step protocol, consisting of V1 (pre-dissection vagus nerve stimulation), R1 (initial RLN stimulation), R2 (post-dissection RLN stimulation), and V2 (post-dissection vagus nerve stimulation), that enables systematic comparison of nerve function before and after thyroid dissection [1]. This protocol helps distinguish global signal loss, which may indicate equipment malfunction or a proximal nerve injury, from focal signal change related to the surgical field.
A key concept in interpreting IONM data is loss of signal (LOS), defined as an electromyographic (EMG) amplitude below 100 ┬ĄV following an initially satisfactory V1 signal (amplitude╦ā500 ┬ĄV), with adequate stimulation at 1-2 mA and after systematic troubleshooting [1,3]. LOS carries prognostic significance for postoperative vocal fold function and directly influences intraoperative strategy, particularly the decision to proceed with contralateral thyroidectomy [3]. However, LOS is a descriptive electrophysiological event, not a diagnosis. It encompasses both true neural LOS, in which actual nerve damage abolishes the EMG response, and false-positive LOS, in which a technical or pharmacological cause produces absent signals despite an intact nerve. When studies report LOS incidence, these two categories are often combined. G├╝r et al. [4] reported LOS in 5.4% of 456 monitored nerves, but the proportion attributable to technical failure versus true injury varied. Published LOS rates range from approximately 3% to over 20%, reflecting differences in study populations, monitoring protocols, and whether post-troubleshooting or pre-troubleshooting events are counted [3,4].
The present review focuses specifically on the technical and pharmacological causes that produce false-positive LOS or otherwise unreliable EMG signals, collectively termed IONM failure in this article. This is distinct from the separate concept of false-negative monitoring, in which satisfactory intraoperative signals fail to predict postoperative vocal fold dysfunction. False-negative events reflect the inherent predictive limitations of IONM rather than equipment or protocol failure, and their detailed discussion falls outside the scope of this review [1,4].
When IONM fails technically, functional feedback is lost: unnecessary staged operations may follow a false-positive LOS in planned bilateral thyroidectomy, or clinician confidence in the technology may erode after repeated unreliable readings [5]. The causes of such failure are multifactorial, encompassing endotracheal tube (ETT) malposition, residual neuromuscular blockade (NMB), equipment and setting errors, and technique-specific challenges in robotic and transoral endoscopic surgery [3,6]. As a narrative rather than systematic review, this article provides a clinically oriented overview of these common causes and discusses preventive and corrective strategies for each, without attempting a formal meta-analysis or exhaustive evidence grading. The major causes of technical IONM failure and their practical preventive or corrective strategies are summarized in Table 1.
Endotracheal Tube Electrode Malposition
1. Mechanism and clinical relevance
ETT malposition is commonly reported as a leading cause of technical IONM failure [3,6]. Standard IONM relies on surface electrodes embedded on the ETT, which require stable, symmetric contact with both vocal folds. Displacement of the tube moves the electrodes away from the glottic plane, reducing or abolishing the recorded EMG amplitude independently of nerve function, a situation that mimics true LOS.
The most frequently described mechanism is cephalad tube migration during the transition from the neutral intubation position to the neck-extended thyroid surgical position. Tsai et al. [7] measured ETT displacement ranging from 16 mm cephalad to 4 mm caudad after neck extension, with a predominant upward shift. The magnitude depends on individual factors including neck length, cervical spine flexibility, and the degree of extension. Initial tube placement depth, tube size relative to the airway, and fixation technique also influence the likelihood of displacement.
Progressive migration during surgery adds further risk. Loosening of fixation tape, the weight of the anesthesia circuit pulling on the tube, and surgical traction on the trachea can shift the tube incrementally, producing gradual signal degradation that becomes apparent during the later stages of the procedure, particularly during R2 and V2 measurements. Rotational malposition along the tube's longitudinal axis disrupts symmetric electrode-vocal fold contact without necessarily being visible externally.
2. Proposed solutions
Performing tracheal intubation after the patient has been placed in the final neck-extended position eliminates displacement caused by subsequent position changes. Direct laryngoscopy in the extended position typically provides a limited glottic view, but Won et al. [8] demonstrated that video laryngoscopy improved glottic visualization in the thyroid surgical position, supporting its use for this purpose.
After positioning, electrode impedance should be checked (target below 5 k╬®) to confirm adequate electrode-tissue contact [3]. Tube depth should be marked at the incisors, and fixation should be reinforced. If signal quality deteriorates intraoperatively, tube position should be reassessed before any conclusions about nerve function are drawn.
Neuromuscular Blockade Management
1. Impact of neuromuscular blockade on intraoperative neuromonitoring
Nondepolarizing NMB agents such as rocuronium inhibit vocalis muscle depolarization by competitive antagonism at the neuromuscular junction [9]. During complete NMB, recordable EMG responses are absent. Even partial residual blockade reduces EMG amplitudes below diagnostic thresholds, creating unreliable readings that may be misinterpreted as neural LOS. Empis de Vendin et al. [10] reported that 12.5% of patients undergoing monitored thyroidectomy required sugammadex reversal to obtain an adequate V1 signal, though routine reversal was not mandatory in the majority who achieved sufficient spontaneous recovery before nerve stimulation.
2. Rocuronium dose and reversal strategy
The degree and duration of laryngeal muscle blockade correlate with the rocuronium dose administered at induction. Lu et al. [11] compared 0.3 mg/kg with 0.6 mg/kg in a randomized trial and found that the lower dose permitted earlier EMG signal recovery, at the cost of slower onset and a lower rate of immediately satisfactory intubating conditions. The clinical trade-off is between ensuring reliable airway management and minimizing residual NMB at the time of first nerve stimulation; the appropriate choice depends on patient-specific airway factors and the anticipated interval from induction to V1.
When residual NMB prevents adequate signal acquisition, pharmacological reversal may be considered in coordination with the anesthesiology team. The available agents differ in mechanism and profile. Neostigmine, an acetylcholinesterase inhibitor, is inexpensive and widely available. Oh et al. [12] showed in a randomized trial that neostigmine administered immediately after intubation shortened the interval to successful V1 stimulation compared with no reversal, without increasing bucking events. Its limitations include a ceiling effect at deep blockade levels, variable reversal kinetics, and the need for anticholinergic co-administration.
Sugammadex encapsulates rocuronium directly, providing faster and more predictable reversal [13]. Lu et al. [14] confirmed that sugammadex at 2 mg/kg adequately restored EMG signals for IONM in a porcine model. In clinical practice, however, the 2 mg/kg dose, commonly used for moderate NMB reversal in the general anesthetic context, has been associated with intraoperative bucking when applied for early IONM-directed reversal. Chai et al. [15] compared 1 mg/kg with 2 mg/kg in a randomized trial and found that bucking occurred less frequently with the lower dose (13.7% versus 35.3%, p=0.020), while monitoring quality did not differ between groups. These single-center findings suggest that a lower sugammadex dose warrants consideration when the objective is partial reversal sufficient for IONM rather than complete reversal for extubation, though confirmation in broader settings is needed.
The waiting interval before rocuronium re-administration after sugammadex depends on the sugammadex dose, the intended re-dose, and renal function, and should follow current labeling guidance rather than a fixed universal time period [13]. The choice between neostigmine and sugammadex, as well as dose and timing, should be individualized according to neuromuscular monitoring status, the expected interval from induction to V1, institutional practice, anesthetic judgment, and patient-specific factors.
Alternative Laryngeal Recording Electrodes
ETT-based surface electrodes remain the standard recording method for IONM, but their signal quality is inherently sensitive to tube position. Alternative laryngeal electrodes, fixed to the laryngeal framework rather than the ETT, have been investigated as complementary options for reducing position-dependent signal variability in selected cases.
Wu et al. [16] evaluated transcartilage surface recording electrodes (adhesive electrodes placed on the outer surface of the thyroid cartilage) in a porcine model and demonstrated stable EMG recordings with less signal variation during tracheal displacement compared with ETT electrodes. In a clinical series, Jung et al. [17] applied transcartilaginous needle electrodes inserted through the thyroid cartilage and reported higher and more stable EMG amplitudes across all four IONM steps compared with simultaneous ETT recordings, along with improved positive predictive value for LOS detection, though the sample was limited to 54 nerves at risk. In a separate study of 105 nerves, Aygun et al. [18] found that cricothyroid muscle electrodes yielded higher amplitudes for EBSLN monitoring than either thyroid cartilage or ETT electrodes, while thyroid cartilage electrodes performed best for vagus and RLN stimulation.
These results are encouraging, but several limitations temper their clinical applicability. Transcartilaginous needle insertion is an invasive step that carries a risk of local bleeding and becomes technically difficult in patients with calcified thyroid cartilage [17]. Electrode placement is operator-dependent, and no standardized positioning protocol has been widely adopted. The existing evidence derives primarily from single-center studies with moderate sample sizes. Additionally, the added procedural time and cost-effectiveness relative to ETT-based monitoring in routine cases have not been formally evaluated. Alternative electrodes should therefore be viewed as complementary adjuncts for selected situations, such as patients with tracheostomies, small-diameter ETTs, or persistent tube-related signal failure, rather than replacements or routine substitutes for standard ETT-based monitoring.
Equipment and Setting Errors
Equipment-related failures range from disconnected cables to incorrect monitor settings. Individually uncommon, they collectively account for a non-negligible share of clinically relevant troubleshooting episodes and are entirely correctable once identified. Their relative brevity in the literature should not imply low clinical importance; a systematic approach to equipment verification is essential for distinguishing technical artifact from true neural events.
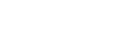
The INMSG troubleshooting algorithm [1,3] recommends a stepwise evaluation when unexpected signal change occurs. The logical starting point is stimulation delivery: the probe tip must be clean, undamaged, and delivering the intended current (1-2 mA for both RLN and vagus nerve stimulation [1]), as contact with electrocautery can compromise probe integrity. Functionality can be verified by stimulating an exposed muscle and observing a visible twitch. If stimulation is confirmed, attention turns to the grounding electrode, since a displaced or poorly conducting ground raises circuit impedance globally and attenuates the recorded signal regardless of nerve status. Recording electrode contact then requires verification: for ETT electrodes, this means reassessing tube position and checking impedance values (target ╦é5 k╬® per electrode); for needle or alternative electrodes, insertion depth and wire integrity should be confirmed. Cable connections between the electrodes, junction box, and monitor also warrant physical inspection, since partially disconnected or loosely seated connectors are a frequently overlooked cause of intermittent signal dropout. Finally, monitor settings should be reviewed: the event detection threshold, sensitivity, and stimulation parameters should match the institutional protocol, with the standard LOS criterion for RLN monitoring, an EMG amplitude below 100 ┬ĄV from an initial satisfactory baseline, serving as a reference [3].
Only after this sequence has been completed without identifying a correctable cause should signal loss be attributed to a neural event. Contralateral vagus stimulation, when available, provides an additional system check: a normal contralateral response in the setting of ipsilateral signal loss supports a true ipsilateral neural event rather than a global equipment failure [1]. Figure 1 summarizes a stepwise approach to troubleshooting unexpected IONM signal loss before attributing the event to true neural injury.
Challenges in Robotic and Transoral Endoscopic Thyroidectomy
Remote-access thyroid surgery, including transaxillary robotic thyroidectomy and transoral endoscopic thyroidectomy vestibular approach (TOETVA), introduces procedure-specific sources of IONM difficulty that extend beyond those encountered through conventional cervicotomy [6,19,20]. The evidence base for monitoring in these approaches is growing but remains more limited than for open surgery, and the considerations described below should be understood as practical precautions rather than established standards.
In robotic approaches, the stimulating probe reaches the target nerve through a longer tissue corridor. Contact between the probe and metal retractors, pooled irrigation fluid, or blood can divert stimulating current away from the nerve, reducing the recorded EMG response. Insulated stimulating probes with a small exposed tip concentrate current delivery. Keeping the operative field dry before each stimulation event further reduces the risk of current dispersion.
TOETVA presents additional challenges related to the proximity of the surgical corridor to the oral cavity and ETT. Saliva tracking along instruments or pooling in the subplatysmal space creates conductive pathways that disperse stimulating current or introduce electrical noise at the recording electrodes [19,20]. Preoperative administration of an antisialagogue such as glycopyrrolate, periodic suctioning of the oral cavity and surgical field, and gauze barriers between the oral and surgical compartments have been described as practical countermeasures [19]. The extent to which these measures eliminate conductive interference has not been rigorously quantified, and awareness of this artifact potential remains important when interpreting equivocal signals during TOETVA.
The longer operative times typical of remote-access procedures also increase the cumulative risk of gradual ETT displacement. Periodic verification of tube position and signal quality, particularly before critical dissection near the RLN, is advisable in these cases. Representative studies supporting the preventive and corrective strategies discussed in this review are summarized in Table 2.
Conclusion
Technical and pharmacological IONM failure during thyroid surgery may produce false-positive LOS or unreliable EMG signals. If unrecognized, these events may lead to unnecessary changes in operative strategy. The principal causes, including ETT electrode displacement, residual NMB, equipment malfunction, and approach-specific signal interference, are individually well described and largely preventable. Intubation after neck extension with laryngoscopic confirmation of electrode position, individualized NMB dosing and reversal, a structured stepwise equipment troubleshooting sequence, and attention to the specific conditions of robotic thyroidectomy and TOETVA together form a practical framework for reducing avoidable monitoring failure. Despite these limitations, ETT-based electrodes remain the current standard recording method for routine thyroid IONM. Alternative laryngeal electrodes may provide supplementary recording options in selected cases, but further standardization and validation are required before broader routine adoption.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




